Avascular necrosis
- Loss of blood supply to femoral head
- Symptoms: decreased hip ROM, groin/thigh pain, antalgic gait
- Diagnosis: clinical, X-ray, bone scan, CT/MRI
Trochanteric bursitis
- Inflammation of trochanteric bursa (often from IT band irritation)
- Symptoms: lateral hip pain, worsens with activity, tenderness
- PT: phase-based intervention (acute/subacute/chronic)
Iliotibial band tightness
- Tight IT band, abnormal gait, may cause trochanteric bursitis
- Symptoms: lateral knee pain, worse with activity, positive Ober’s/Noble’s tests
- PT: gait training, pain reduction, soft tissue/manual techniques
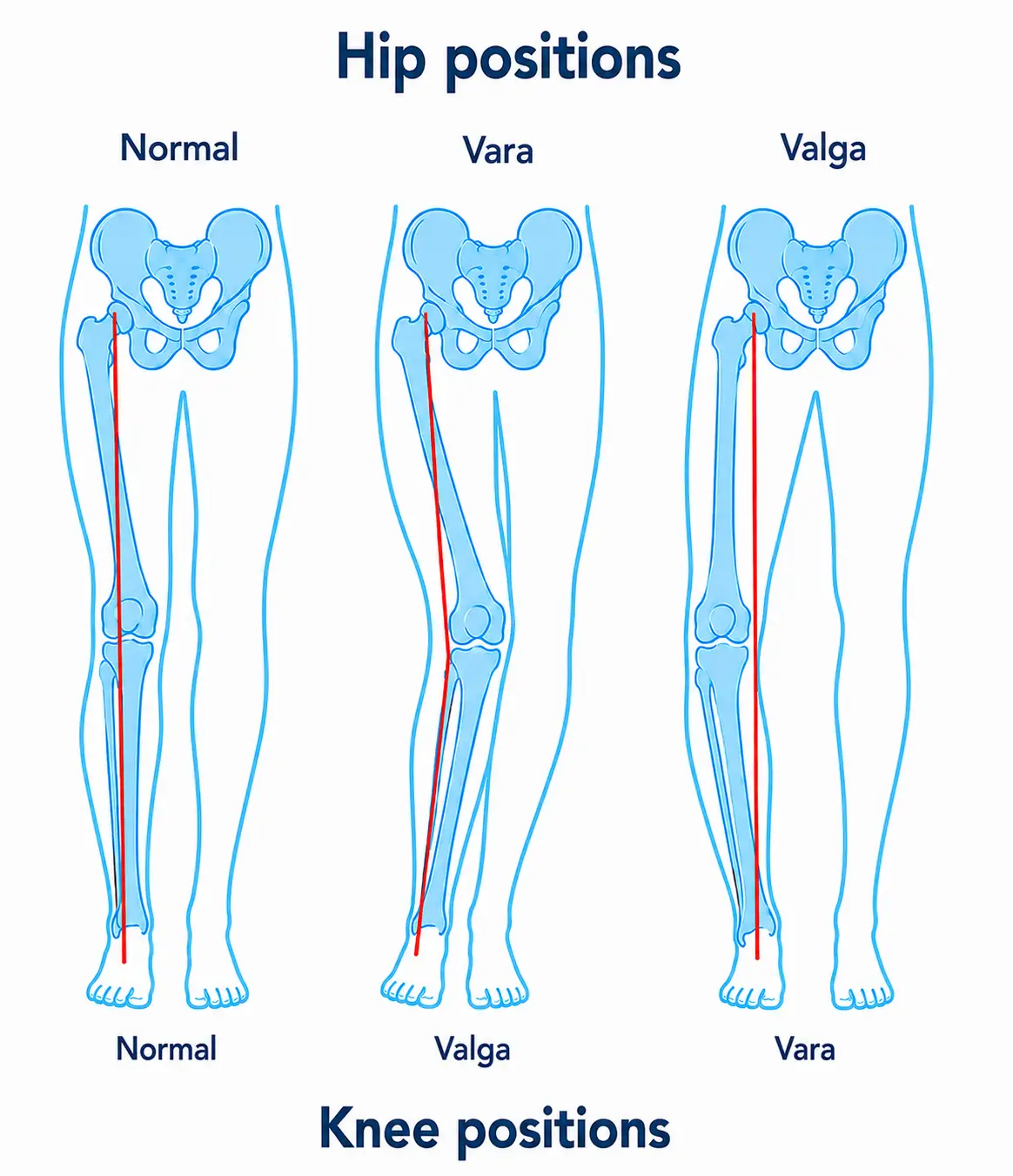
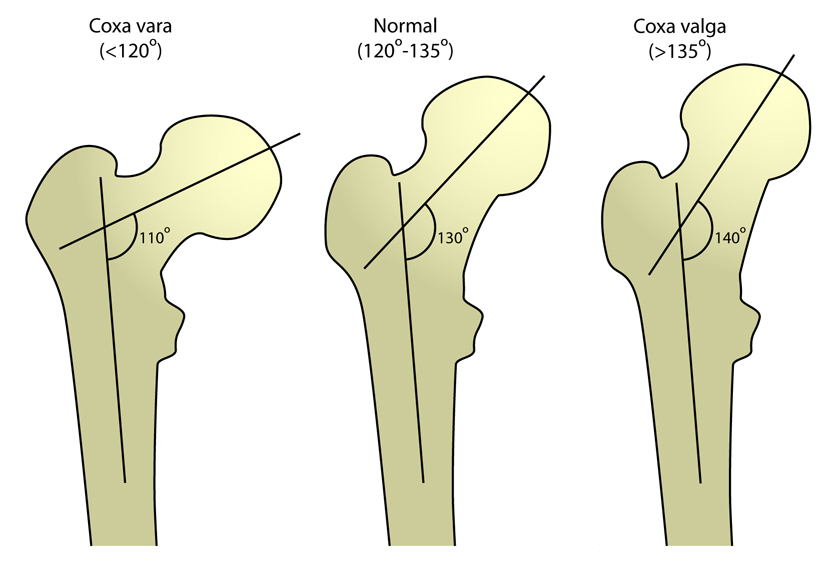
Coxa vara and coxa valga
- Abnormal femoral neck angles (<115° vara, >125° valga)
- Symptoms: leg length discrepancy, hip pain, limited mobility (vara); increased anterior pelvic tilt (valga)
- PT: joint mobility, orthotics, muscle energy techniques
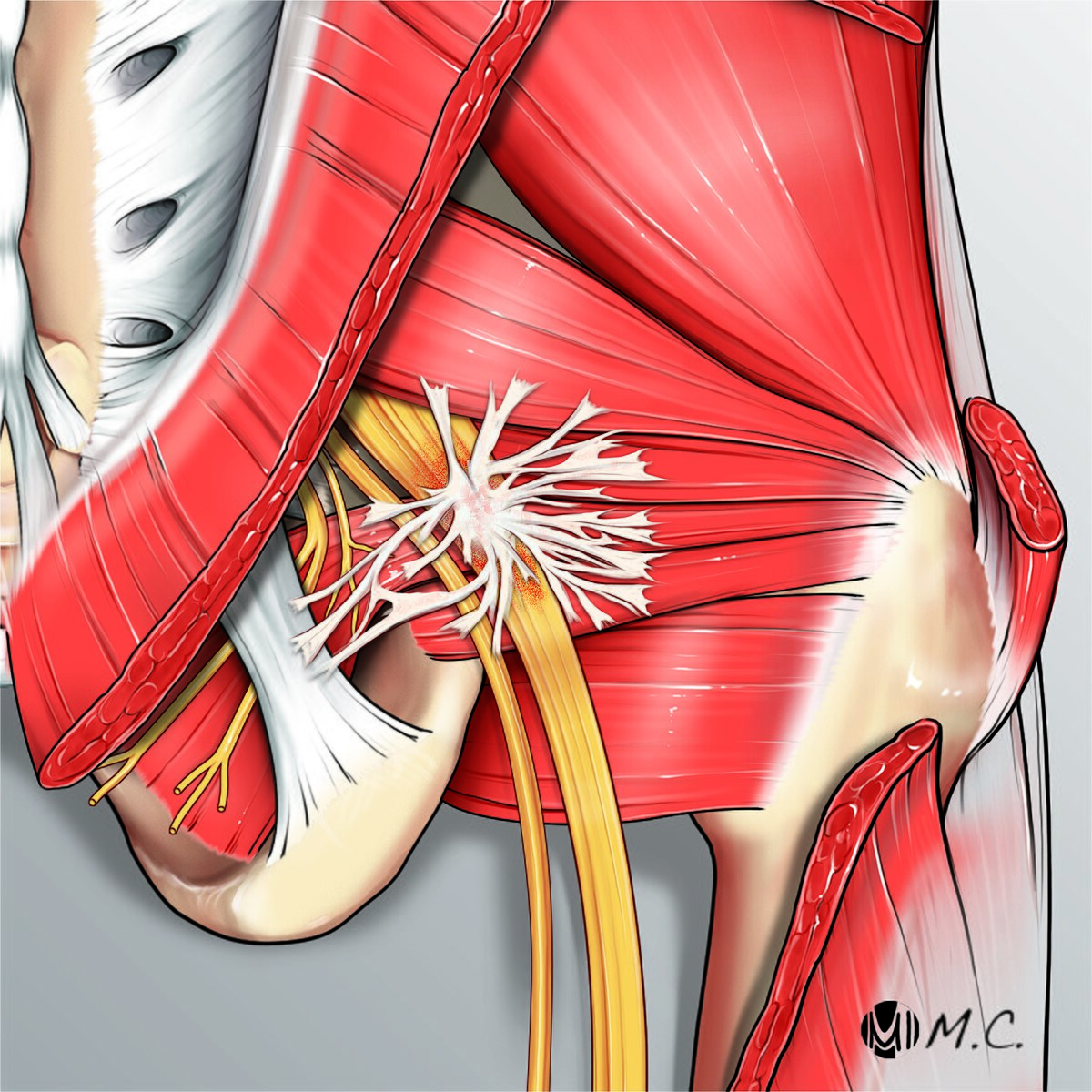
Piriformis syndrome
- Piriformis tightness/spasm compresses sciatic nerve
- Symptoms: pain radiating down leg, restricted internal rotation, piriformis tenderness
- PT: pain centralization, muscle mobility/strengthening, biomechanical correction
Ligament sprains (knee)
- Involves ACL, PCL, MCL, LCL; graded I–III by severity
- Diagnosis: special tests (Lachman, drawer, valgus/varus), MRI
- PT: pain/inflammation reduction, functional/joint training, post-surgical protocols
Meniscus injuries
- Caused by flexion, compression, rotary knee forces
- Symptoms: pain with twisting/weight-bearing, locking/giving way
- Diagnosis: McMurray, Apley, Thessaly tests; MRI
Patellofemoral pain syndrome
- Dysfunction from trauma, muscle imbalance, improper loading
- Symptoms: anterior knee pain, worse with stairs/squatting, grinding sensation
- PT: pain reduction, patella taping/mobilization, biofeedback for vastus medialis
Patellar tendinopathy
- Degeneration of patellar tendon (overload/jumping)
- Symptoms: activity-related anterior knee pain, tenderness, abnormal patella position (alta/baja)
- PT: strengthen quads/hamstrings, patella taping/bracing
Acute compartment syndrome (lower leg)
- Increased compartment pressure (trauma/fracture)
- Symptoms: six P’s (pain, pallor, pulselessness, paresthesia, paresis, palpable tenderness)
- Medical emergency: immediate fasciotomy
Chronic exertional compartment syndrome
- Gradual increased compartment pressure (repetitive activity)
- Symptoms: pain, numbness, weakness, swelling, foot drop
- PT: activity modification, proprioceptive/functional training
Stress fractures
- Microfractures of tibia/fibula (overuse, poor alignment)
- Symptoms: dull pain, swelling, worse with activity/rest
- Diagnosis: X-ray, MRI
Ligament sprains (ankle/foot)
- Graded I–III (mild to severe tear)
- Symptoms: swelling, pain, bruising, instability (grade-dependent)
- PT: RICE, functional training, joint protection, post-surgical protocols
Achilles tendinopathy
- Chronic Achilles tendon inflammation (overuse, RA, gout)
- Symptoms: posterior heel pain, stiffness, swelling, worse with activity
- PT: phase-based intervention (acute/chronic)
Tarsal tunnel syndrome
- Posterior tibial nerve entrapment in tarsal tunnel
- Symptoms: numbness/tingling sole/arch, burning pain, foot drop
- Diagnosis: Tinel’s sign, electrodiagnostics
Foot deformities (pes cavus, equinus)
- Pes cavus: high arch; equinus: plantarflexed foot
- Causes: genetics, biomechanical faults, neuro conditions
- PT: biomechanical alignment, orthoses, joint mobility
Charcot-Marie-Tooth disease
- Progressive peroneal muscular atrophy (genetic)
- Symptoms: foot/leg weakness, high arches, numbness, muscle atrophy
- PT: education, skin assessment, contracture prevention, mobility training
Foot deformities (rearfoot/forefoot varus/valgus)
- Rearfoot varus: calcaneal inversion; valgus: eversion
- Forefoot varus: forefoot inversion; valgus: eversion
- PT: foot alignment, orthoses, strengthening