







Special tests of the spine, pelvis, and temporomandibular joint
Special tests spine and pelvis
Cervical spine
- Vertebral artery test
- The examiner carefully extends the patient’s neck, then rotates the head to one side and holds it there for up to 30 seconds. The patient’s eyes are kept open and monitored, and they are usually asked to count backward or speak to check for changes in their voice.
- Tests the integrity of the vertebrobasilar vascular system
- Positive: symptoms of dizziness, dysphagia, diplopia, nystagmus- red flag, and the therapist does not progress with any movements of the cervical spine
- Vertebral artery test should always be performed before cervical spine mobilization- if not performed, this is considered sub-standard care and can be life-threatening
- The examiner carefully extends the patient’s neck, then rotates the head to one side and holds it there for up to 30 seconds. The patient’s eyes are kept open and monitored, and they are usually asked to count backward or speak to check for changes in their voice.
- Flexion rotation test
- Patient in supine with maximal flexion of neck performed with rotation to left and right
- Provocative test for atlantoaxial dysfunction or cervicogenic headache
- Positive: reproduction of headache symptoms or loss of 10 degrees of mobility when comparing left and right rotation (when compared to each side)
- Patient in supine with maximal flexion of neck performed with rotation to left and right
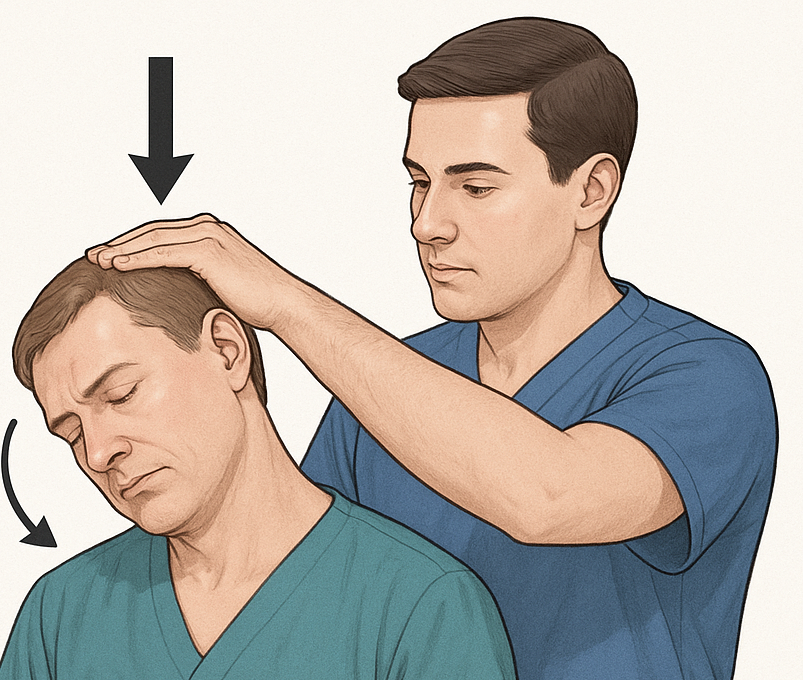
- Spurling’s test (foraminal compression)
- Patient sitting with head laterally bending towards the involved side while the therapist applies pressure straight down
- Confirms cervical root dysfunction
- Positive: pain and paresthesia in a dermatomal pattern of the cervical root
- Patient sitting with head laterally bending towards the involved side while the therapist applies pressure straight down
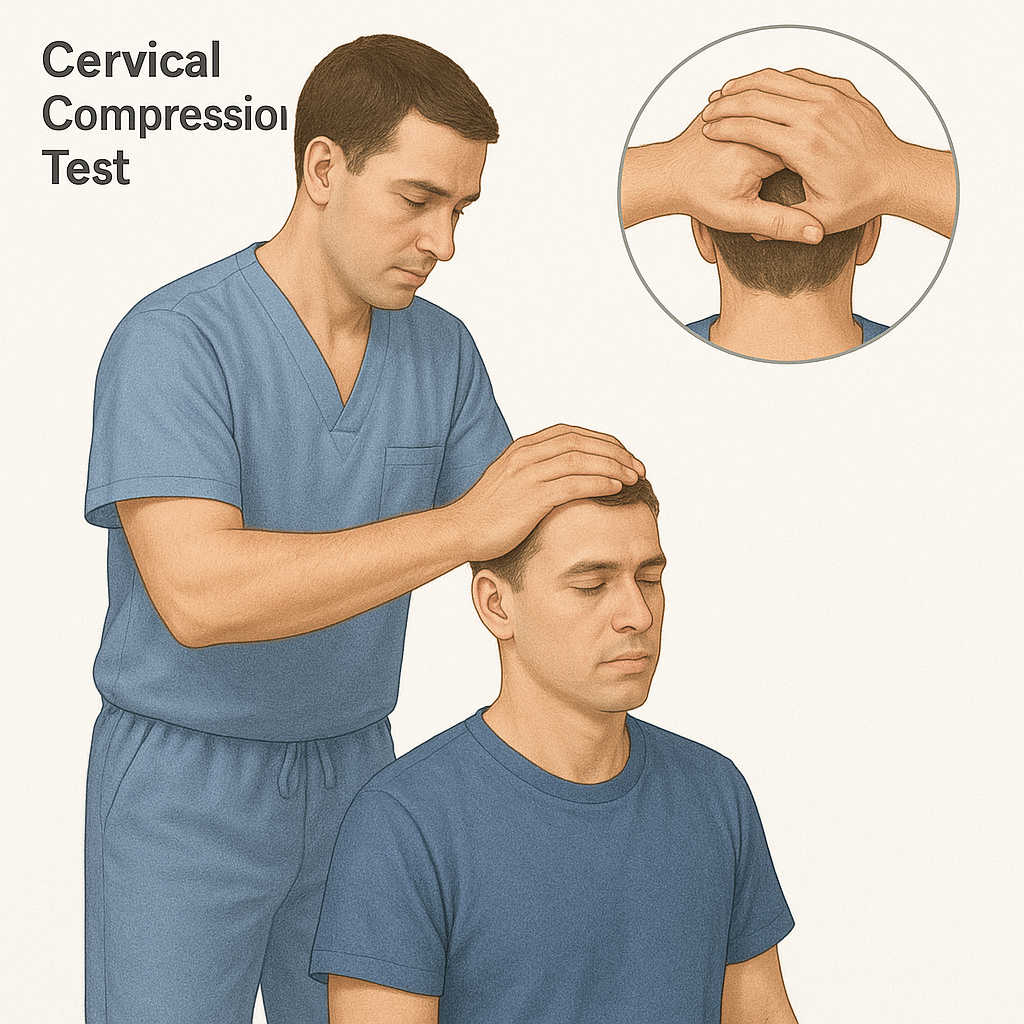
- Cervical compression test
- Patient sitting and neck passively moved into lateral flexion and rotation to the non-painful side, followed by extension. Repeat the painful side.
- Identifies intervertebral foramen and/or facet dysfunction
- Positive: pain and paresthesia in a dermatomal pattern of cervical root or localized pain in the neck if facet dysfunction
- Patient sitting and neck passively moved into lateral flexion and rotation to the non-painful side, followed by extension. Repeat the painful side.
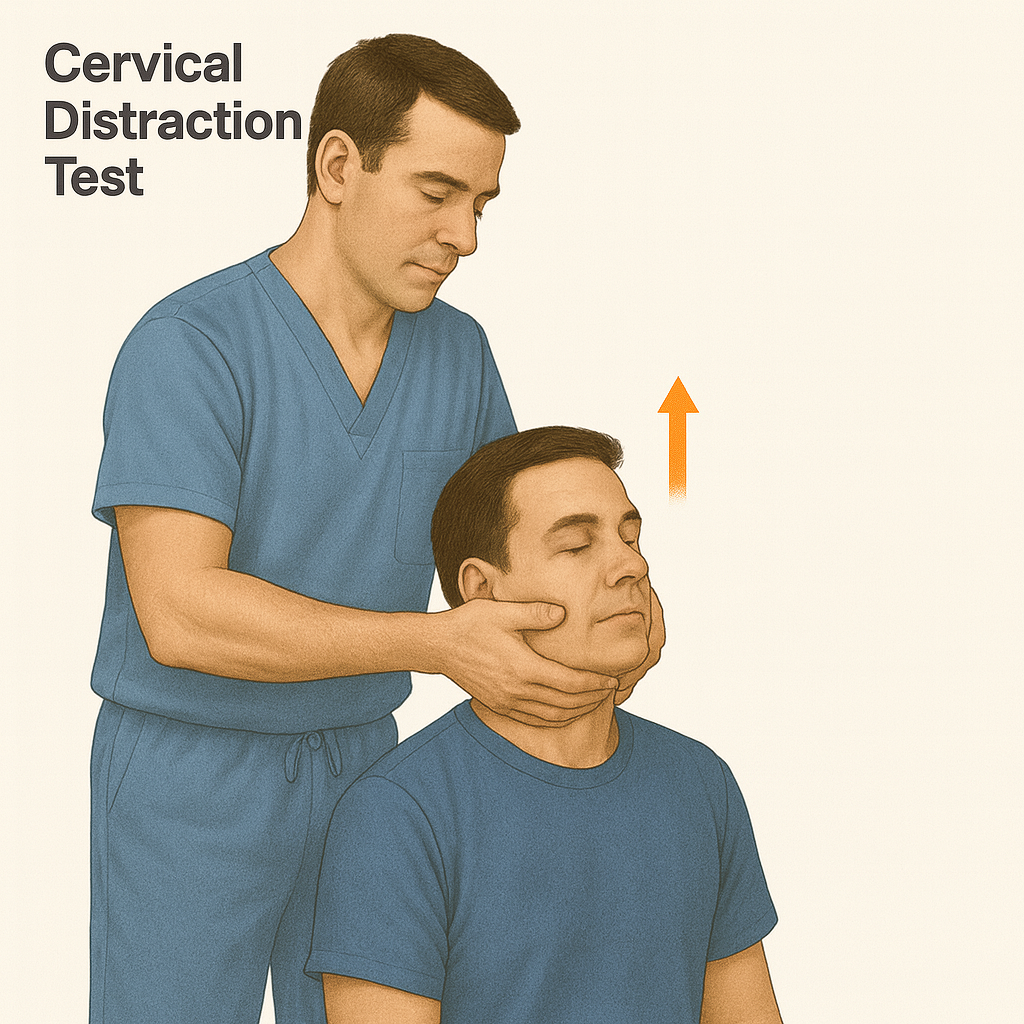
- Distraction test
- Patient sitting with head passively distracted
- Identifies intervertebral foramen and/or facet dysfunction
- Positive: decrease in symptoms or decrease in upper limb pain
- Patient sitting with head passively distracted
- Lhermitte’s sign
- Patient long sitting on mat; therapists passively flex the patient’s head and hip while keeping the knee in extension. Repeat with the other hip.
- Identifies upper motor neuron lesions (often associated with multiple sclerosis)
- Positive: electrical pain down the spine and into the upper or lower limbs
- Patient long sitting on mat; therapists passively flex the patient’s head and hip while keeping the knee in extension. Repeat with the other hip.
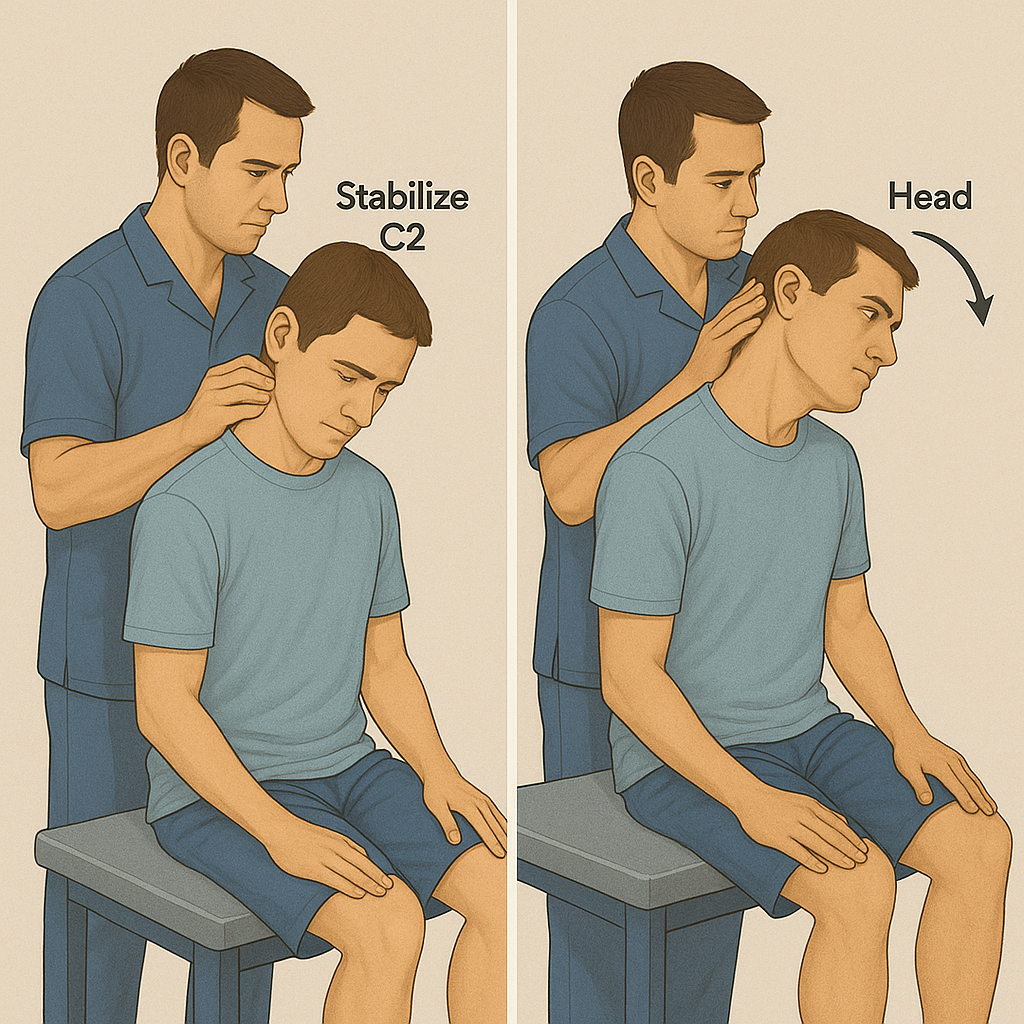
- Alar ligament test
- Patient seated and therapist palpates C2 spinous process; the therapist passively flexes the upper cervical spine with lateral flexion and rotation
- Tests the integrity of the alar ligament
- Positive: Inability to palpate C2 and/or inability to feel movement at C2
- Patient seated and therapist palpates C2 spinous process; the therapist passively flexes the upper cervical spine with lateral flexion and rotation
Thoracic spine scoliosis screening
- Adam’s Forward Bend Test:
- The child bends forward at the waist while keeping their knees straight.
- Checks for any asymmetry or curvature in the spine.
- The child bends forward at the waist while keeping their knees straight.
- Positive: elevation of the ribs on one side of the spine
Lumbar spine
-
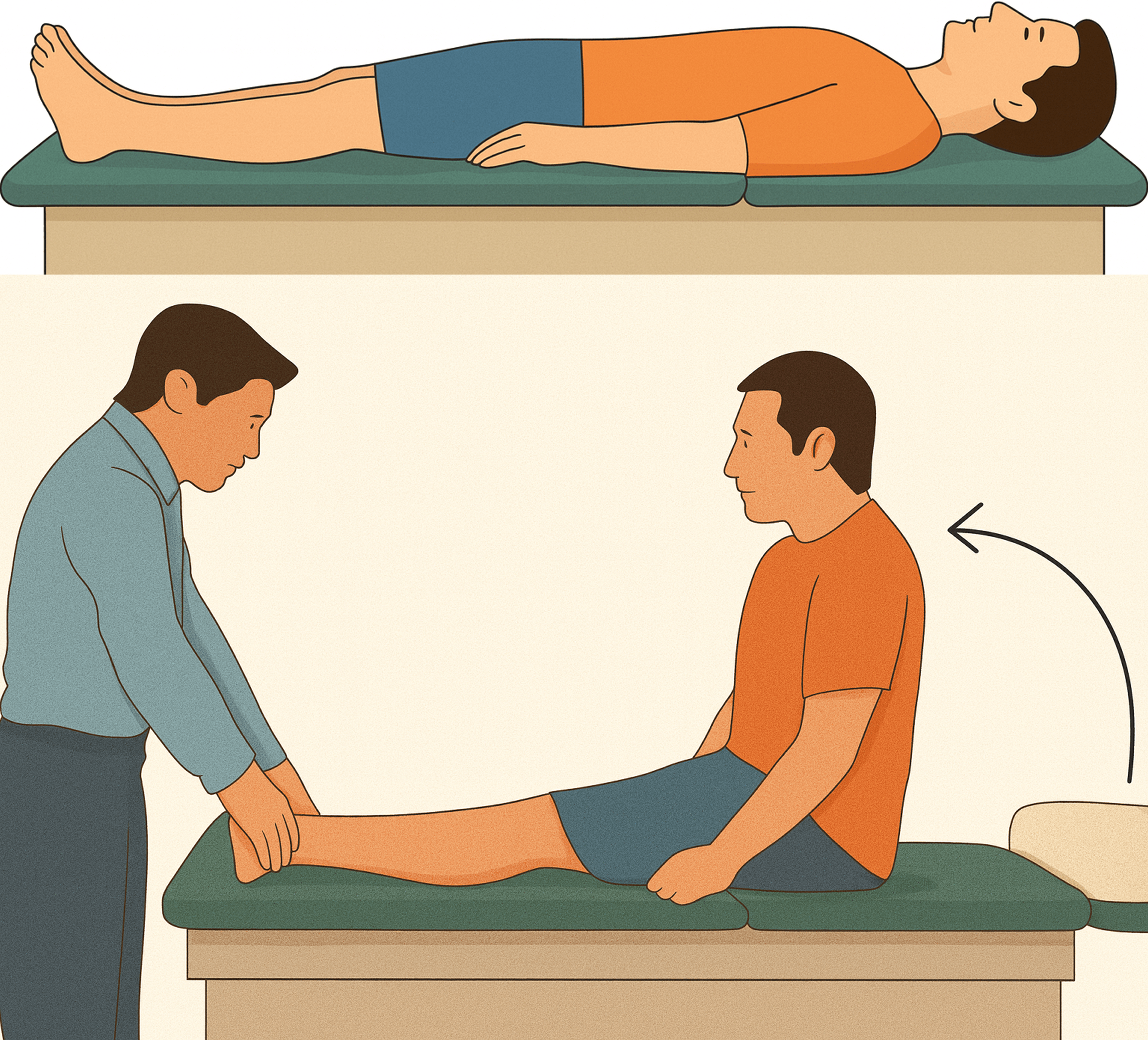
Slump test
- Patient sits with knees flexed and neutral neck and head; progress through the following steps- passively flex head and neck, passively extend knee, passively dorsiflex ankle of limb- repeat with opposite leg
- The therapist will stop at a step if reproduction of symptoms occurs
- Tests for neurological dysfunction of the lower extremity
- Positive: pain, paresthesias, numbness/tingling, and other neurological symptoms detects disc herniations, or screen for sciatica by placing the nervous system under tension,
- The therapist will stop at a step if reproduction of symptoms occurs
- Patient sits with knees flexed and neutral neck and head; progress through the following steps- passively flex head and neck, passively extend knee, passively dorsiflex ankle of limb- repeat with opposite leg
-
Prone instability test
- Patient prone with torso supported on the mat, legs off the edge, with both feet supported on the ground. The therapist applies posterior/anterior springing throughout the lumbar spine to identify painful segments. The therapist then instructs the patient to lift the legs off the floor and perform the me posterior/anterior springing
- Tests the instability of the lumbar spine
- Positive: decreased pain during posterior/anterior springing with the legs raised compared to when the feet are supported on the ground. This means the instability is neuromuscular rather than purely structural, clinical lumbar instability.
- Patient prone with torso supported on the mat, legs off the edge, with both feet supported on the ground. The therapist applies posterior/anterior springing throughout the lumbar spine to identify painful segments. The therapist then instructs the patient to lift the legs off the floor and perform the me posterior/anterior springing
-
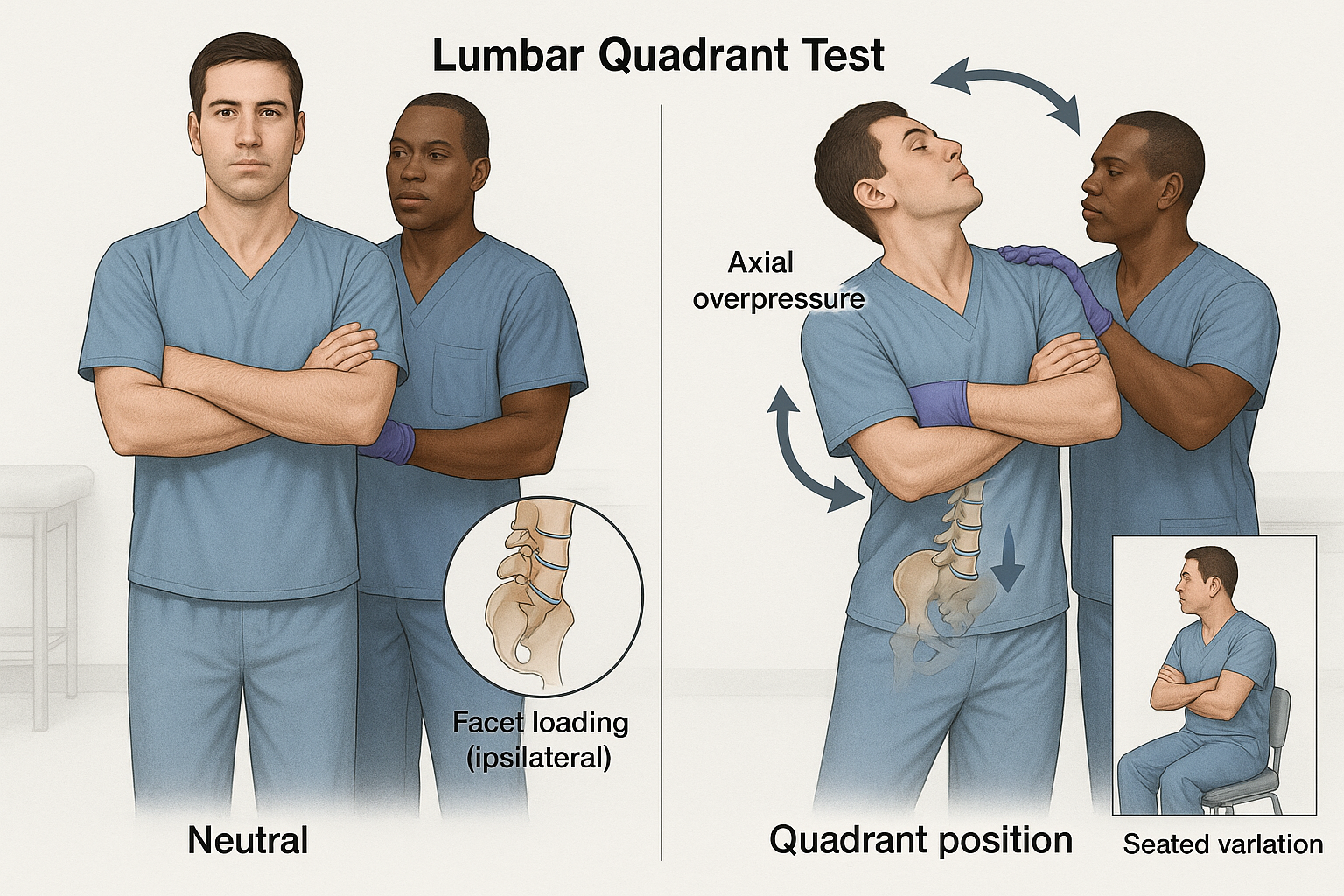
Lumbar Spine Quadrant Test (Kemp’s Test)
- Patient standing
- The patient stands and is guided by the practitioner to maximally extend their spine, then rotate and laterally flex toward the side of the pain. The practitioner applies a gentle downward pressure
- Tests the compression of neural structures at the facet and intervertebral foramen
- Positive: pain or paresthesias in a dermatomal pattern or localized pain if facet dysfunction
- Patient standing
Neurological dysfunction
- Lower limb tension tests assist with identifying peripheral nerve injury by placing the lower limb in positions that will stress the nerve
- Prone knee flexion with hip extension tests femoral nerve
Sacroiliac
- Long sitting
- Patient supine with therapist palpating the medial malleolus- therapist observes alignment. The therapist then asks the patient to come to a long sitting position to observe if alignment at the medial malleolus is still present.
- Tests for leg length discrepancy due to the sacroiliac joint
- Positive: one leg observed longer when coming to a long sitting position compared to the supine position
- Patient supine with therapist palpating the medial malleolus- therapist observes alignment. The therapist then asks the patient to come to a long sitting position to observe if alignment at the medial malleolus is still present.
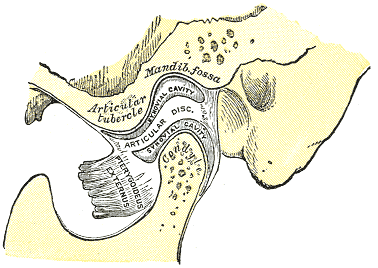
Temporomandibular joint (TMJ)
- Elevation (Closing):
- Contraction of the masseter, temporalis, and medial pterygoid muscles raises the mandible.
- Depression (Opening):
- Relaxation of the elevator muscles and contraction of the digastric, geniohyoid, and mylohyoid muscles lowers the mandible.
- Protrusion (Forward Movement):
- Contraction of the lateral pterygoid muscles moves the mandible forward.
- Retrusion (Backward Movement):
- Contraction of the posterior fibers of the temporalis muscles moves the mandible backward.
- Lateral Deviation (Side-to-Side Movement):
- Contraction of the lateral pterygoid muscle on one side moves the mandible toward that side.
Special tests of TMJ
- TMJ compression
- Patient sitting or supine; therapist stabilizes the patient’s head with one hand while the other hand pushes the mandible superiorly, causing a compressive load to the TMJ
- Assess pain in the retrodiscal tissues
- Positive: pain in the TMJ
- Patient sitting or supine; therapist stabilizes the patient’s head with one hand while the other hand pushes the mandible superiorly, causing a compressive load to the TMJ