Gait
Normal patterns of gait
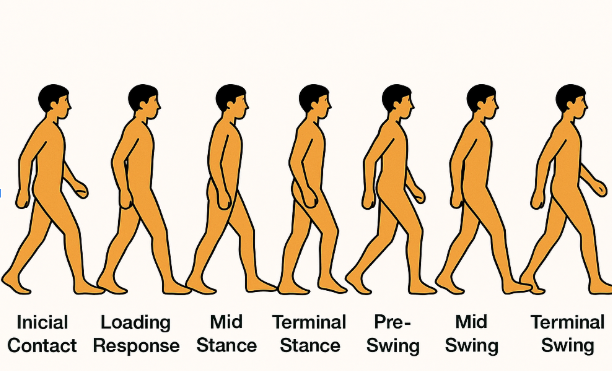
Phases of the gait cycle
- Stance phase — 60% of the cycle
- Swing phase — 40% of the cycle
Stance phase (will be denoted as traditional/Rancho Los Amigos terminology)
- Heel strike/initial contact
- The beginning of the stance phase, when the heel or another part of the foot contacts the ground
- Joint positions: hip flexion, knee extension, ankle 0 degrees dorsiflexion
- Muscles activated
- Erector spinae — eccentric
- Gluteus maximus — concentric
- Quadriceps — eccentric
- Hamstrings — concentric
- Anterior tibialis — eccentric
- Extensor digitorium longus — eccentric
- Flexor digitorium longus — eccentric
- Foot flat/loading response
- The portion of the first double support period of the stance phase from the initial contact until the contralateral extremity leaves the ground
- Joint positions: hip flexion, knee flexion, ankle 15 degrees plantarflexion
- Muscles activated
- Erector spinae- concentric
- Gluteus maximus- concentric
- Gluteus medius/minimus/tensor fasciae latae- concentric (closed chain to stabilize pelvis for opposite side swing phase).
- Quadriceps - eccentric
- Anterior tibialis- eccentric (toe to prevent foot slap)
- Extensor digitorium longus- eccentric
- Flexor digitorium longus - eccentric
- Muscles activated
- Midstance/midstance
- The portion of the single limb support stance phase that begins when the contralateral extremity leaves the ground & ends when the body is directed over the supporting limb
- Joint positions: hip extension, knee extension, ankle 0 degrees dorsiflexion (allows for the highest point in the gait cycle).
- Muscles activated
- Iliopsoas- eccentric
- Gluteus medius/minimus/TFL- concentric (closed chain to stabilize pelvis for opposite side swing phase)
- Hamstrings- eccentric
- Gastrocnemius-eccentric
- Muscles activated
- Heel off/terminal stance
- The last portion of the single limb support stance phase that begins with heel rise and continues until the contralateral extremity contacts the ground
- Joint positions: hip hyperextension, knee extension, ankle 15 degrees dorsiflexion * Muscles activated * Iliopsoas- eccentric * Gluteus medius/minimus/TFL- concentric (closed chain to stabilize pelvis for opposite side swing phase) * Hamstrings- concentric * Gastrocnemius- concentric
- Toe off/ preswing
- The portion of stance that begins the second double support period from the initial contact of the contralateral extremity to lift off the reference extremity
- Joint positions: hip flexion, knee flexion, ankle 10 degrees plantarflexion
- Muscles activated
- Iliopsoas- concentric
- Adductor magnus- concentric
- Hamstrings- concentric
- Quadriceps- eccentric
- Anterior tibialis- concentric
- Gastrocnemius- concentric
- Muscles activated
Swing phase (will be denoted as traditional/Rancho Los Amigos terminology)
- Acceleration/initial swing
-
The portion of swing from the point when the reference extremity leaves the ground to the maximum knee flexion of the same extremity
-
Joint positions: hip flexion, knee flexion, ankle 0 degrees plantarflexion
- Muscles activated
- Iliopsoas- concentric
- Hamstrings- concentric
- Quadriceps- eccentric
- Anterior tibialis- concentric
- Muscles activated
-
- Mid-swing
- Portion of the swing phase from maximum knee flexion of the reference extremity to a vertical tibial position
- Joint positions: hip flexion, knee flexion, approx. 65 degrees, ankle 0 degrees plantarflexion (maximal shortening of the limb for ground clearance).
- Muscles activated
- Iliopsoas — concentric
- Hamstrings — eccentric
- Anterior tibialis — concentric
- Muscles activated
- Deceleration/terminal swing
- The portion of the swing phase from a vertical position of the tibia of the reference extremity to just before initial contact
- Joint positions: hip flexion, knee extension, ankle 0 degrees plantarflexion
- Muscles activated
- Iliopsoas — concentric
- Hamstrings — eccentric
- Anterior tibialis — concentric
- Muscles activated
Gait assessment
Keys to a thorough gait assessment:
- Observe the patient walking: Watch them walk towards and away from you, noting their overall gait pattern, speed, and stability.
- Look for abnormalities: Pay attention to any deviations from normal gait, such as:
- Uneven stride length: One leg appears to take shorter or longer steps than the other.
- Foot placement: Observe how the heel and toes make contact with the ground.
- Arm swing: Note the presence and symmetry of arm movement.
- Pelvic movement: Look for any unusual or excessive pelvic tilting or rotation.
- Trunk sway: Observe excessive or abnormal trunk movement during walking.
- Assess balance: Observe how the patient maintains balance during walking and turning.
- Evaluate speed: Note whether the patient walks at a normal or unusual speed.
- Evaluate endurance: Observe signs of fatigue or difficulty maintaining gait over a distance.
Primary gait muscles and actions
Important gait terms
- Femoral anteversion: medial rotation of femur
- Can be related to the medial rotation of the tibia, toe in
- Femoral retroversion: lateral rotation of femur
- Can be related to lateral rotation of the tibia, toe out
- Internal tibial torsion: medial rotation of femur
- Can be related to toe in
- External tibial torsion: lateral rotation of femur
- Can be related to toe out
- Genu valgum: knock-knees
- Can be related to internal tibial torsion
- Genu varum; bowlegged
- Can be related to external rotation
Abnormal gait
- Common swing phase compensation
- Result of apparent or actual leg length discrepancies.
- Hip hike or shrug
- Hip circumduction
- Steppage gait
- Common stance phase compensation
- Result of apparent or actual leg length discrepancies.
- Vaulting (hyperextending the knee and plantarflexing the ankle)
Antalgic (painful) gait
- Result of injury to the pelvis, hip, knee, ankle, or foot.
- The stance phase on the affected leg is shorter than that on the unaffected leg, because the patient attempts to remove weight from the affected leg as quickly as possible.
- Example: L knee pain — the stance phase of L is shortened.
- This causes shortened L stride length.
- This will cause longer R stride length
- Example: L knee pain — the stance phase of L is shortened.
Ataxic gait
- Results from neurological deficits resulting in abnormal walking patterns characterized by poor coordination and balance, most often associated with cerebellar dysfunction
- Typically presents with clumsy, staggering movements with a wide-based gait
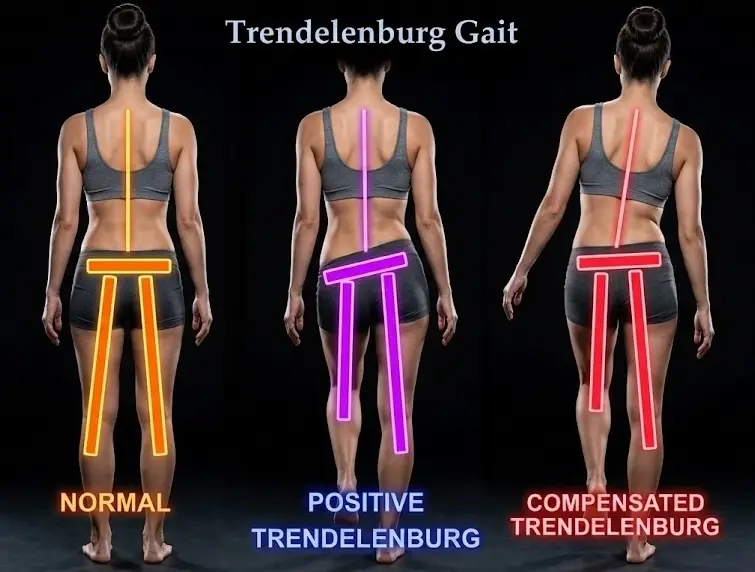
(Gluteus medius Trendelenburg) gait
-
Weakness of the gluteus medius causes an abnormal gait pattern. The weakness always involves the stance leg with an inability to stabilize the pelvis and a drop of the pelvis on the swing leg, or compensated by leaning over the weak stance leg.
- Increased lateral lean over the affected side
- Dropped hip over unaffected side
- Hip hike on affected side
Hemiplegic or hemiparetic gait
- Results from weakness or flaccidity in an affected extremity, leading to various gait deficits
- Examples of hemiparetic gait patterns are: hip weakness or flaccidity may cause circumduction gait during the swing phase of gait, or anterior tibialis weakness could cause foot slap gait during the initial contact of gait
Steppage or drop foot gait
- Weak or paralyzed anterior tibialis muscles cause the foot to drag across the ground during the swing phase of gait.
- Inability to clear the ground during the mid-swing phase of gait because of loss of control of the anterior tibialis muscle due to weakness or innervation.