Dislocations of the glenohumeral joint caused by traumatic or atraumatic reasons
Trauma is due to direct injury
Atramautic can be due to repetitive injury causing hypermobility
Types of dislocations:
Anterior-inferior dislocations: caused by excessive abduction and external rotation of upper extremity with subsequent disruption in inferior glenoid ligament, anterior capsule, and glenoid labrum
If traumatic can lead to:
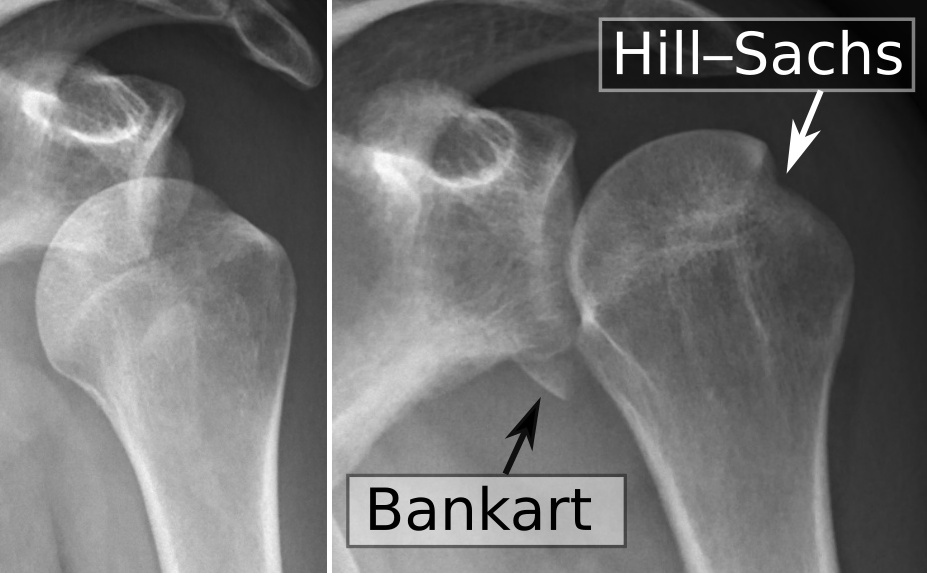
Hills-sachs lesion: compression fracture of posterior humeral head
Superior labrum, anterior to posterior tear (SLAP)
Bankhart lesion: avulsion of the anterior-inferior capsule and glenoid labrum
Axillary nerve injury: numbness, tingling, and weakness in deltoid
Hills sachs and Bankart lesions
Posterior dislocations : rare, caused by horizontal adduction and internal rotation
Labral tears
Tear in the cartilage ring that surrounds the shoulder joint; divided into above the middle of the socket and below the middle of the socket
Above the middle of the socket is caused a SLAP (superior labral anterior-posterior) tear; can also involve the biceps tendon
Below the middle of the socket is caused a Bankhart lesion; can also involve the inferior glenoid ligament
Labral tears are associated with traumatic injury or repetitive shoulder dislocations
Rotator cuff tendonitis
Caused by mechanical impingement of the distal attachment of the rotator cuff causing inflammation of the tendons
Increased risk for development of tendonitis due to poor vascularity at attachment sites
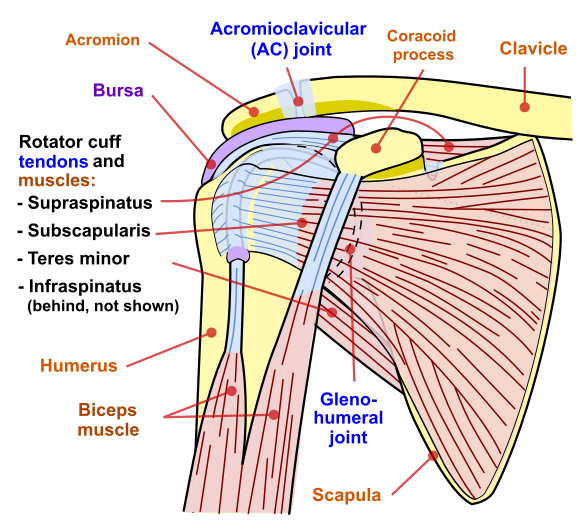
Shoulder joint
Impingement syndrome
Impingement (entrapment) of rotator cuff tendon against the acromion due to mechanical repetition
Adhesive capsulitis
Restriction in shoulder motion due to inflammation of the joint capsule
Restrictions are in external rotation (greatest), abduction and flexion (capsular pattern of shoulder)
Reason for diagnosis can be repetitive motion, diabetes, cardiovascular disease, or thyroid disease
Acromioclavicular and sternoclavicular disorders
Occurs when fall on adducted shoulder or when with collision with another individual particularly during sporting event
Grades of injury
Type I
A minor sprain of the acromioclavicular ligament
No radiographic displacement
No tear of the acromioclavicular or coracoclavicular ligament
Type II
A tear of the acromioclavicular ligament, but not the coracoclavicular ligaments
Less than 25% increase in the coracoclavicular interspace
Type III
Tears of both the acromioclavicular and coracoclavicular ligament
25% to 100% displacement of the clavicle
Type IV
Tears of both the acromioclavicular and coracoclavicular ligament
Posterior displacement of the distal clavicle into the trapezius fascia
Subacromial/subdeltoid bursitis
Subacromial and subdeltoid burse become inflamed (close relationship with rotator cuff tendonitis )
The bursa becomes trapped (impinged) beneath the acromion arch
Bicepital tendonitis
Inflammation of the long head of the biceps
Cases can be mechanical trapping (impingement) of the long head of biceps between acromion and bicipital groove of humerus
Proximal humeral fracture
Occurs due to fall on outstretched arm
Stable fractures that do not require surgery
Distal humeral fracture
Trauma causes fracture at distal humerus
Immediate attention must be given to if supracondylar fracture due to increased likelihood of neurovascular involvement
Radial nerve involvement and vascular structures may lead to paralysis and/or pulselessness
In children, can cause malunion due to growth plate involvement
Lateral epicodyle fractures will require internal fixation (rod and screws implanted in arm) for proper alignment
Thoracic outlet syndrome
Compression of neurovascular bundle to that includes the brachial plexus, sympathetic trunk, subclavian artery and vein, and phrenic and vagus nerves due to alteration in thoracic outlet size
Common areas of compression are:
Superior thoracic outlet
Scalene triangle
Between clavicle and first rib
Between pectoralis minor and thoracic wall
Elbow differential diagnosis
Medial epicondylitis
Inflammation of the pronator teres and the flexor carpi radialis tendons at the attachment of at the medical epicondyle
Typically due to overuse in activities that require excessive pronation at the forearm
Commonly referred to as golfer’s elbow
Lateral epicondylitis
Inflammation of the extensor carpi radialis brevis tendon at its attachment at the lateral epicondyle
Gradual onset occurring with repetitive wrist extension resulting in overloading of the extensor carpi radialis
Ulnar collateral ligament injuries
Due to repetitive valgus stress to medial elbow causing stress to ulnar collateral ligament
Elbow dislocation
Caused by trauma to the elbow causing misalignment from anatomical position
Posterior dislocation is the most common
Posterolateral dislocation occurs as a result of hyperextension from a fall on outstretched arm
Posterior dislocations commonly cause avulsion fracture of medial epicondyle
Complete dislocation will impact all of the following structures
Tightness of pronator teres muscle and under superficial head of flexor digitorum superficialis secondary to repetitive gripping activities
Symptoms
Pain, numbness, tingling, and weakness in median nerve distribution in forearm and below
Diagnosis
Clinical presentation
Manual muscle test of forearm muscles
Positive Tinel’s test in median nerve distribution
Radial nerve entrapment
Entrapment of posterior interosseous nerve within radial tunnel as a result of overhead activities and throwing
Symptoms
Lateral elbow pain
Pain, numbness, tingling, and weakness in radial nerve distribution in forearm and below
Diagnosis
Clinical presentation
Manual muscle test of forearm muscles
Positive Tinel’s test in radial nerve distribution
Ulnar nerve entrapment
Compression or trauma at cubital tunnel, thickened retinaculum or hypertrophy of flexor carpi ulnaris muscle
Symptoms
Medial elbow pain
Pain, numbness, tingling, and weakness in ulnar nerve distribution in forearm and below
Diagnosis
Clinical presentation
Manual muscle test of forearm muscles
Positive Tinel’s test in ulnar nerve distribution
Medial management for all nerve entrapments
Acetaminophen or non-steroidal inflammatory (NSAIDs)
Physical therapy management for all nerve entrapments
Early interventions- rest, modalities to reduce inflammation/pain
Wrist and hand differential diagnosis
Carpal tunnel syndrome
Compression of the of the median nerve at the carpal tunnel at the wrist due to inflammation of the wrist flexor tendon or inflammation of the median nerve
Caused by repetitive wrist motions; other causes may be pregnancy, diabetes, or rheumatoid arthritis
deQuervain’s tenodsynovitis
Inflammation of the extensor pollics brevis and abductor pollics longus
Due to repetitive microtrauma or can occur during pregnancy
Colles fracture
Fracture causing posterior displacement of distal radius with radial shift of wrist and hand
Most common fracture from falling out on outstretched hand
Can cause median nerve damage if edema is unmanaged
Scaphoid fracture
Due to fall onto outstretched arm
This is the most common fractured carpal bone
Dupuytren’s contracture
Contracture of the palmar fascia leading to flexion of the digits towards the palm
Common in the metacarpalphalangeal (MCP and proximal interphalangeal (PIP) joints of fourth and fifth digits in nondiabetic and third and fourth in diabetic
Swan neck deformity
Contracture of intrinsic muscles with dorsal subluxation of lateral extensor tendons
Commonly occurs after trauma to hand or with diagnosis of rheumatoid arthritis
Deformity noted is flexion of MCP and DIP with extension of PIP
Mallet finger
Rupture or avulsion of extensor tendon at its insertion into distal phalanx digit
Commonly occurs after trauma forcing distal phalanx into a flexed position
Deformity noted is flexion of DIP
Ape hand deformity
Median nerve dysfunction causes thenar muscle weakness with first digit moving dorsally until it becomes aligned with second digit
Sign up for free to take 22 quiz questions on this topic