Prosthetics and orthotics
Prosthetics
Levels of amputations
Upper extremity
- Finger or partial hand: Removal of one or more fingers or part of the hand
- Wrist disarticulation: Removal of the hand at the wrist joint
- Transradial (below elbow): Removal of the forearm below the elbow joint
- Elbow disarticulation: Removal of the arm at the elbow joint
- Transhumeral (above elbow): Removal of the arm above the elbow joint
- Shoulder disarticulation: Removal of the arm at the shoulder joint
Lower extremity
- Toe or partial foot: Removal of one or more toes or part of the foot
- Ankle disarticulation: Removal of the foot at the ankle joint
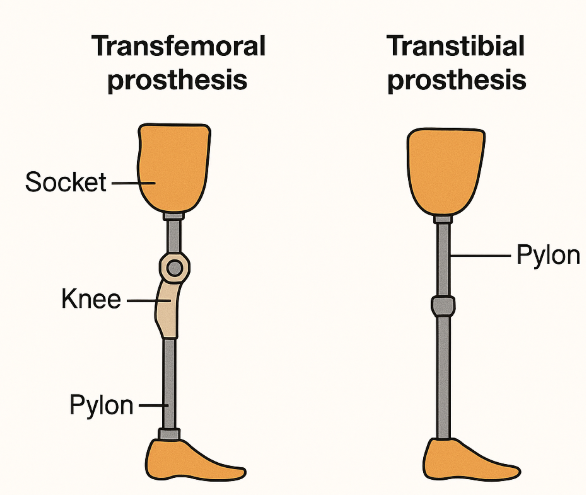
- Transtibial (below knee): Removal of the leg below the knee joint
- Knee disarticulation: Removal of the leg at the knee joint
- Transfemoral (above knee): Removal of the leg above the knee joint
- Hip disarticulation: Removal of the leg at the hip joint
Focus of NPTE is on lower extremity prosthesis
Components of prosthesis
Primary components
- Sockets
- custom-molded prosthetic that will have total contact with residual limb; goal is equal distribution of tissue load throughout the socket
- Liners
- Silicone barrier between residual limb and socket to decrease shear forces
- Socks
- Used to aid in changing the size of the residual limb
- Terminal device
- Interface between prosthetic limb and external environment
- Upper limb: the terminal device is a hand or a hook
- Lower limb: the terminal device is the foot
- Interface between prosthetic limb and external environment
Components of a prosthesis specifically for transtibial amputation
Ankle-foot assembly
- SACH foot (solid ankle cushioned heel):
- A simple, durable, and lightweight foot with a solid ankle joint
- Single-axis foot:
- Features a hinged ankle joint that allows for up-and-down movement, enhancing knee stability.
- Multi-axis foot:
- Similar to a single-axis foot, but also allows for side-to-side movement, making it better suited for uneven terrain
- Microprocessor-controlled (MPC) feet:
- These feet use sensors and a computer to adjust the ankle’s position and resistance based on the user’s movements and the environment
Shank
- Endoskeleton prosthesis:
- Structure: Features a tubular structure connecting the primary components, like the socket, suspension system, foot, and knee unit
- Appearance: Often covered with cosmetic foam
- Advantages: Endoskeletal prostheses are adjustable and lighter than exoskeletal prostheses.
- Disadvantages: Less durable than exoskeletal prostheses
- Exoskeleton prosthesis:
- Structure: Has a hard outer shell that provides structural strength and cosmetic shape
- Materials: Traditionally constructed from wood or plastic
- Durability: More durable than endoskeletal prostheses
- Advantages: May be preferred by people who do physical labor or are in harsh environments
- Disadvantages: Less customizable than endoskeletal prostheses.
Socket
- Patellar tendon bearing (PTB) sockets:
- Focus: PTB sockets, often used for below-knee amputations, focus weight-bearing stress on pressure-tolerant structures like the patellar tendon and medial tibia flare
- Advantages:
- Can be a good choice for patients with shorter or bony residual limbs
- Easier to don/doff for amputees with poor hand dexterity, poor eyesight, or hemiparesis
- Can be modified to accommodate changes in the residual limb after amputation
- Disadvantages:
- May not be ideal for patients with residual limb scar tissue or chronic skin breakdown
- Advantages:
- Focus: PTB sockets, often used for below-knee amputations, focus weight-bearing stress on pressure-tolerant structures like the patellar tendon and medial tibia flare
- Total surface bearing (TSB) sockets:
- Focus: TSB sockets, also used for below-knee amputations, distribute weight evenly across the entire limb surface, reducing pressure points
- Advantages:
- Often used with gel liners, which cushion the limb and protect the skin, making them great for amputees with scar tissue or sensitive skin
- Offer better suspension than PTB designs, often using locking pins or suction systems
- Disadvantages:
- Can be more difficult to don/doff than PTB sockets
- Advantages:
- Focus: TSB sockets, also used for below-knee amputations, distribute weight evenly across the entire limb surface, reducing pressure points
Components of prosthesis specifically for transfemoral amputation
Knee unit
- Single-axis knees:
- Mechanism: A single pivot point, resembling a simple hinge.
- Stability: Offers good stability during the stance (weight-bearing) phase but may require more effort for the swing (forward movement) phase
- Suitable for individuals with lower activity levels, those who can voluntarily stabilize the knee
- Types:
- Manual Locking: The knee can be locked in extension for stability, and unlocked manually for sitting
- Constant Friction: Provide a constant resistance to knee flexion during the swing phase, aiding in stability
- Polycentric (multiaxis) knees:
- Mechanism: Multiple pivot points, allowing for a more natural and efficient gait, particularly during the swing phase.
- Stability: Shorten the prosthesis during swing, reducing the risk of tripping and improving stability.
- Suitable for active individuals, those with longer residual limbs, or those who require a more natural gait.
- Types:
- Hydraulic/Pneumatic: Use fluid or air to control the swing phase, allowing for smoother and more natural movement
- Microprocessor-Controlled: Use of sensors and electronics to adjust the resistance to knee flexion and extension based on the user’s gait and activity level.
- Microprocessor knees:
- Mechanism: Use of sensors and electronics to adjust the resistance to knee flexion and extension based on the user’s gait and activity level.
- Benefits: Improve stability, reduce energy expenditure, and allow for a more natural and comfortable gait
- Suitable for highly active individuals, those who require a high level of stability and control, or those who want to maximize their mobility.
Socket
- Ischial containment (IC) sockets
- These designs feature a narrow medial-lateral dimension with the ischium (part of the pelvic bone) encapsulated within the socket, rather than sitting on the brim
- Sub-ischial sockets
- These sockets have a lower proximal trim line than IC sockets, and are often used with vacuum-assisted suspension
- Quadrilateral (quad) sockets
- These were historically the most common type, but are less common now, although still used for some patients
- Direct socket * A novel method of fabricating a laminated interface directly onto the residual limb
Keys for transfemoral amputation and transtibial amputation
- The posterior and medial walls are lower than the anterior and lateral walls of the socket
- This allows room for the groin and sacrum.
Prosthetic gait deviations
Vaulting
- Definition: An attempt to lengthen the stance phase on the intact limb by knee extension and ankle plantar flexion during mid-stance
- Causes:
- Limb too long
- Poorly suspended prosthesis
- Excessive plantarflexion
Circumduction
- Definition: The prosthetic limb travels in a lateral arch during swing.
- Causes:
- Limb too long
- Poorly suspended prosthesis
- Excessive plantarflexion
Abducted gait pattern
- Definition: The prosthetic limb is carried in an abducted position throughout the swing and stance phase
- Causes:
- Outset prosthetic foot
- Prosthesis too long
- Medially placed intact foot
Knee instability
- Definition: Excessive knee flexion on the prosthetic side in early stance
- Causes:
- Excessive foot dorsiflexion
- Excessive socket flexion
- Posterior translation of foot/pylon
- Excessively hard heel cushion on prosthetic heel
- Weakness of the knee extensors
Reduced toe clearance
- Definition: Prosthetic toe drags or catches during the swing phase
- Causes:
- Prosthetic limb too long
- Inadequate suspension
- Residual limb not getting into prosthetic socket all the way
- Excessive plantarflexion of the prosthetic foot
Pelvic drop
- Definition: The pelvis on the prosthetic side drops on initial contact as if “stepping into a hole.”
- Causes:
- Prosthetic limb too short
- Residual limb has shrunk relative to the socket
- Excessively compliant heel cushion
Lateral trunk lean over prosthesis (Trendelenburg)
- Definition: Trunk bends laterally over the prosthesis (compensated Trendelenburg) during stance
- Causes:
- Inadequate adduction of the socket
- Prosthesis too short
- Outset foot
- Medial wall too high, causing pain
- Gapping at the lateral wall of the socket
Medial/lateral whip
- Definition: Abrupt medial or lateral movement of the prosthetic heel during swing
- Causes:
- Excessive external or internal rotation of the socket
- Socket too tight
- Inadequate suspension
- Excessive valgus of prosthetic knee
Increased knee flexion
- Definition: Long prosthetic step (decreased stance time on prosthesis)
- Causes:
- Painful socket — residual limb; painful
- Prosthesis too long
- Excessive foot dorsiflexion
- Excessively hard heel cushion on prosthetic heel
Orthotics
- Soft orthotics
- Also called accommodative orthotics, these are made of flexible materials that mold to the shape of your foot. They can help with conditions like plantar fasciitis and diabetes-related foot ulcers
- Rigid orthotics
- Also called functional orthotics, these are made of firm materials like plastic or carbon fiber. They can help with foot deformities and repetitive stress injuries
- Semi-rigid orthotics
- These combine soft and rigid materials to provide both cushioning and stability. They are often used for flat feet.
- Sports-specific orthotics
- These are designed for athletes to improve alignment and reduce the risk of injury
Lower limb orthotics
Foot orthoses (FO)
- Definition:
- Foot orthoses are inserts placed inside shoes to support, align, or improve foot function. They help with conditions such as flat feet, plantar fasciitis, and overpronation
- Components:
- Shell: The main body of the orthotic, made from rigid, semi-rigid, or soft materials
- Posting: Adjustments to correct alignment (e.g., medial wedge for overpronation)
- Top Cover: Soft padding for comfort and shock absorption
- Heel Cup: Helps control heel motion and provides stability
- Arch Support: Maintains the natural arch to prevent excessive collapse
- Types:
- Rigid FO: Controls foot motion and alignment, typically made of plastic or carbon fiber.
- Semi-Rigid FO: Provides balance between control and flexibility, often used in sports
- Soft FO: Offers cushioning for diabetic patients or those with sensitive feet
Ankle-foot orthoses (AFO)
- Definition:
- Ankle-foot orthoses (AFOs) extend from the foot to just below the knee and are used for conditions affecting foot and ankle stability, such as drop foot, stroke, cerebral palsy, and peripheral neuropathy
- Components:
- Footplate: Extends under the foot to control foot movement
- Ankle Joint: Can be fixed, hinged, or adjustable to allow varying degrees of movement
- Straps: Secure the orthosis to the leg for stability
- Calf Support: Provides additional control over ankle motion
- Material: Typically made from thermoplastics, carbon fiber, or metal uprights for different levels of support
- Types:
- Solid AFO: Provides complete immobilization of the ankle joint
- Hinged AFO: Allows controlled ankle motion while still providing support
- Carbon Fiber AFO: Lightweight and energy-efficient for active users
- Specific types of AFO
- Other types:
- Posterior leaf spring AFO: A flexible
- An AFO that helps with foot clearance during walking by providing a spring-like effect AFO with a posterior stop: A physical block on the back of the brace that prevents excessive ankle plantar flexion for controlling an unstable knee**
- Carbon fiber AFO: A lightweight and strong AFO made of carbon fiber, offering good support and durability
- Dynamic ankle foot orthosis (DAFO): Designed for individuals with neurological conditions, often shorter, and with a neurological footplate design
- Ground reaction force ankle foot orthosis (GRAFO): Designed to reduce instability at the knee joint as well as the foot and ankle
- Hybrid AFO: A combination of different AFO types, offering a balance of support and flexibility
- Other types:
Knee-ankle-foot orthoses (KAFO)
- Definition:
- Knee-ankle-foot orthoses (KAFOs) extend from the foot to the thigh, providing support for patients with quadriceps weakness, spinal cord injuries, or post-stroke conditions.
- Components:
- Footplate: Provides support to the foot like an AFO
- Ankle Joint: Can be rigid, hinged, or free-motion
- Knee Joints: May include locking mechanisms (drop lock, bail lock) or free-motion for controlled knee flexion
- Thigh Cuff: Provides proximal stability to the femur
- Straps & Padding: Ensure proper fit and comfort
- Materials: Metal (for strong support) or plastic (for lighter weight)
- Types:
- Locked KAFO: Prevents knee flexion for complete knee support.
- Stance control KAFO: Allows free knee flexion during the swing phase but locks during the stance
- Offset joint KAFO: Reduces knee buckling by shifting the mechanical knee joint posteriorly
Hip-knee-ankle-foot orthoses (HKAFO)
-
Definition:
- A hip-knee-ankle-foot orthosis (HKAFO) is a full-leg brace that supports and stabilizes the hip, knee, ankle, and foot. HKAFOs are often prescribed for individuals with significant muscle weakness or paralysis in the lower limbs and hips.
-
Components:
- Footplate: provides support to the foot like an AFO
- Ankle joint: can be rigid, hinged, or free-motion
- Knee joints: may include locking mechanisms (drop lock, bail lock) or free-motion for controlled knee flexion
- Thigh cuff: provides proximal stability to the femur
- Hip joint and pelvic band: controls hip motion and connects the orthosis to the pelvis, sometimes using a pelvic girdle for maximum stability
- Straps and padding: ensure proper fit and comfort
- Materials: metal (for strong support) or plastic (for lighter weight)
-
Types:
- Conventional HKAFOs: offer basic support with different joint options: single-axis, two-position lock, or double-axis hip joints.
- Reciprocating gait orthosis (RGO) is a specialized type of HKAFO. It uses a cable or bar system to couple the hip flexion of one leg with the hip extension of the opposite leg.
- Microprocessor-controlled HKAFOs (MPKAFOs): use microprocessors to regulate swing and stance control, offering stability, stumble recovery, and controlled knee flexion.
Spinal orthoses
Lumbar-Sacral Orthoses (LSO)
- Definition:
- LSOs provide support and stability to the lumbar and sacral spine, commonly used for low back pain, post-surgical stabilization, herniated discs, and fractures
- Components:
- Rigid or Semi-Rigid Frame: Provides stability and restricts motion
- Abdominal Panel: Offers compression to reduce lumbar lordosis
- Straps or Velcro Closures: Ensure a snug fit.
- Pelvic Section: Stabilizes the sacrum and lower lumbar spine
- Types:
- Rigid LSO
- Restricts lumbar flexion and extension.
- Commonly used post-surgery or for fractures.
- Corset-style LSO
- Provides mild to moderate support.
- Often used for chronic back pain and muscle strain
- Jewett brace
- Hyperextension orthoses are designed to limit spinal flexion
- Used for anterior compression fractures
- Rigid LSO
Thoracolumbar-Sacral Orthoses (TLSO)
- Definition:
- TLSOs provide support to the thoracic, lumbar, and sacral spine, commonly used for post-surgical recovery, scoliosis, and compression fractures
- Components:
- Rigid or Semi-Rigid Frame: Limits spinal movement
- Anterior and Posterior Panels: Provide structural support
- Straps for Compression: Adjust tightness for stabilization
- Shoulder Straps (for some models): Helps maintain posture
- Types:
- Rigid TLSO
- Used for scoliosis and spinal fractures.
- Limits motion in all planes.
- Hyperextension TLSO
- Limits spinal flexion but allows extension.
- Common for compression fractures.
- Soft TLSO
- Provides mild support and posture correction.
- Used for mild osteoporosis or muscle strain
- Rigid TLSO
Cervical Orthoses (CO)
- Definition:
- Cervical orthoses are designed to support and immobilize the cervical spine, commonly used for whiplash, post-surgical recovery, and cervical fractures
- Components:
- Collar or shell: Provides cervical stabilization.
- Anterior and Posterior Panels (for rigid braces): Limit flexion, extension, and rotation
- Chin and occipital support: Maintains head position
- Types:
- Soft cervical collar
- Provides minimal support and is used for mild strains or whiplash
- Rigid cervical brace (e.g., Philadelphia Collar, Miami J, Aspen Collar)
- Provides moderate to firm immobilization.
- Common for post-operative care and cervical fractures
- Halo vest orthosis
- Provides maximum cervical immobilization
- Used for unstable cervical fractures or post-surgical fusion
- Sterno-occipital mandibular immobilizer
- Limits flexion and extension, often used for C1-C3 fractures
- Soft cervical collar