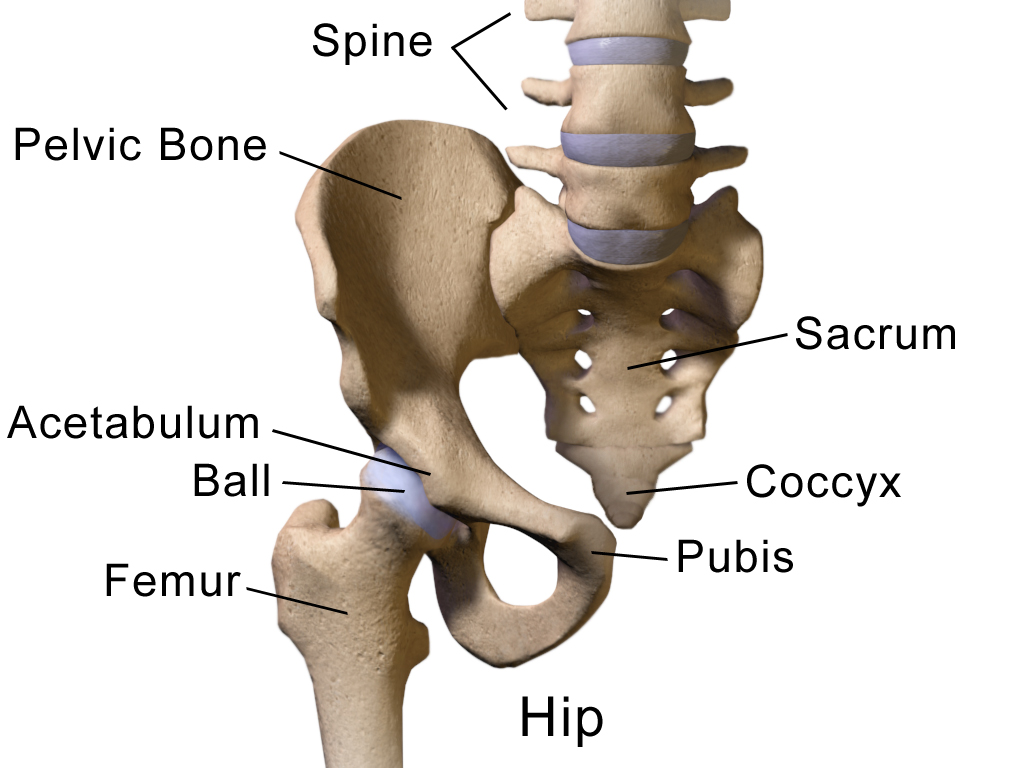
The hip region comprises two (2) bony structures- the acetabulum and femur.
The normal angle of inclination is 115-125 degrees (angel of inclination between femur and acetabulum)- if angle is >125 degree then referred to as coxa valga; if angle is <115 degrees then referred to as coxa varus. Femoral neck angle is positioned anteriorly at a 10-15 degree angle; excessive anterior rotation >25 degrees is anteversion and excessive posterior rotation <10 degrees in retroversion.
The primary movements of the hip are that are:
Hip flexion/ extension
Hip external rotation/ internal rotation
Hip abduction/adduction
The hip joint is a stable synovial joint due to the bony anatomy and strength of ligaments, capsule, and labrum.
Capsule encloses the entire joint
Labrum
Attached to the acetabulum and serves to deepen structure to allow for greater articulation
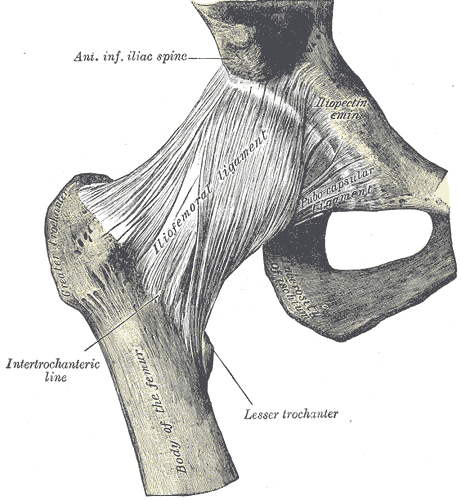
Ligaments
Iliofemoral
Two (2) bands that originate at anterior iliac spine (ASIS), run medially to distal intertrochanteric line and lateral running to proximal aspect of intertrochanteric line
Both bands tighten with extension and external rotation; superior band tight with adduction; inferior band tightens with abduction
Pubofemoral
Band tightens with extension, external rotation, and abduction
Ischiofemoral
Band tightens with medial rotation, abduction, and extension
Other pertinent structures of the hip joint are:
Zona orbicularis- aids in holding head of femur in acetabulum
Inguinal ligament- forms tunnel for vital arteries, veins, and nerves in lower extremity
Bursae- act as fluid-filled sac that provides cushioning and friction reduction between tendons, joints, muscles and bone
Lumbosacral joint
Hip joint
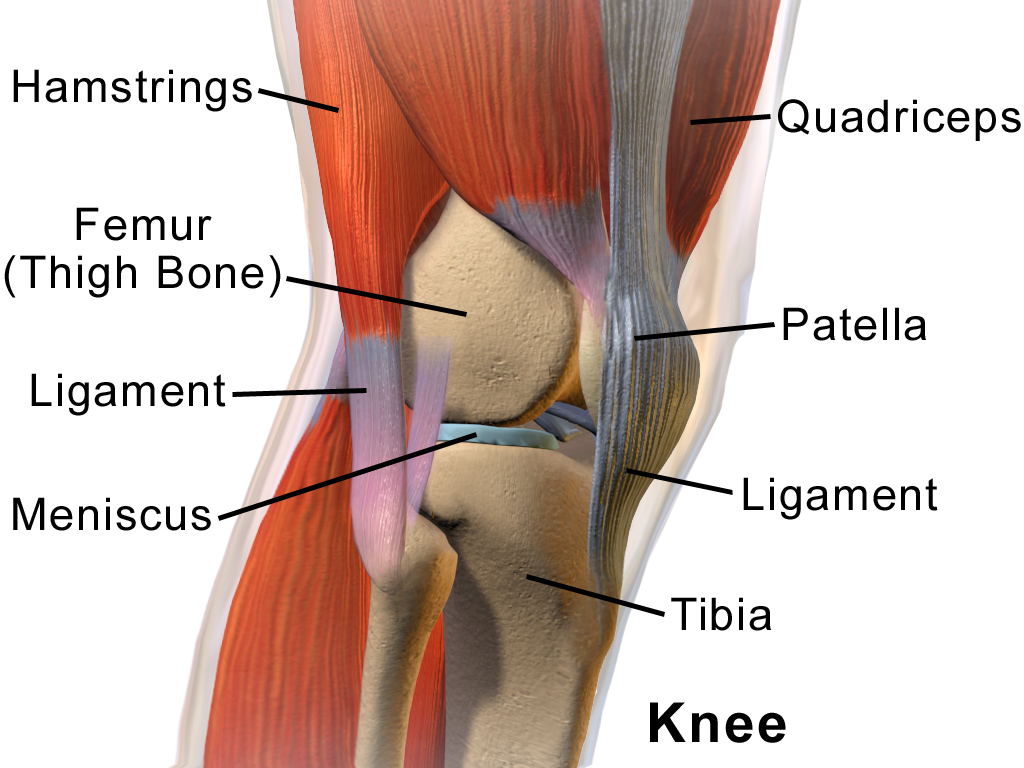
Knee region
The knee region is composed of four (4) bony structures- femur, tibia, fibula, and patella. These bony structures then form three (3) joints- tibiofemoral, patellafemoral, and proximal tibiofibular joint.
Knee joint
The primary movements of the knee that are aided by the three joints of the knee are:
Knee flexion/extension
Other pertinent structures of the knee joint are:
Capsule
Tibiofemoral capsule covers distal femur and proximal tibia- posteriorly divided into medial and lateral sections, anterior cut-out for patella
Proximal tibofibular capsule is continuous with knee 10% of time
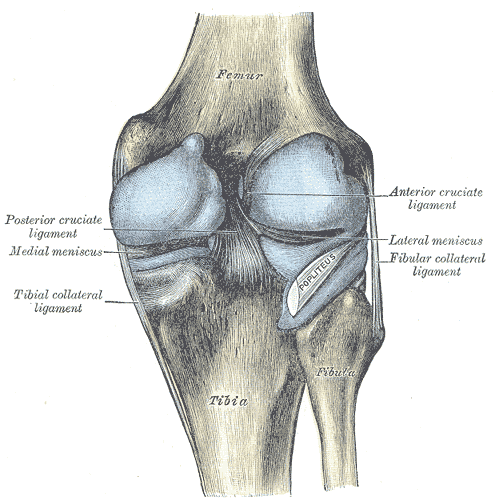
Ligaments
Tibiofemoral and patellofemoral joints
Medial collateral ligament
Tightened in extension; slackened in flexion
Prevents internal rotation and provides stability against valgus forces
Lateral collateral ligament
Tightened in extension; slackened in flexion
Prevents external rotation and provides stability against varus forces
Anterior cruciate ligament
Prevents anterior displacement of tibia on femur and provides rotation stability
Posterior cruciate ligament
Prevents posterior displacement of tibia on femur
Meniscofemoral ligament
Aids posterior cruciate ligament in preventing posterior displacement of tibia on femur
Transverse ligament
Connects medial and lateral meniscus anteriorly
Alar fold
Keeps patella in contact with tibia
Proximal tibiofibular joint ligaments
Anterior tibiofibular ligament
Reinforces anterior capsule
Posterior tibiofibular
Reinforces posterior capsule
Menisci
Function
Deepen fossa of tibia
Increased congruency of tibia and femur
Reduces friction between joints during movement
Improves weight distribution
Provides shock absorption and lubrication to knee
Provide stability to tibiofemoral joint
Lateral meniscus
Outer side of joint
Attached to popitieus and joint capsule
Stabilizes knee against lateral rotation and tibial rotation
Medial meniscus
Inner side of joint
Attached to medial collateral ligament and joint capsule
Stabilizes knee against medial rotation and tibial translation
Bursae- act as fluid-filled sac that provides cushioning and friction reduction between tendons, joints, muscles and bone
Ligaments of knee
Posterior view of ligaments
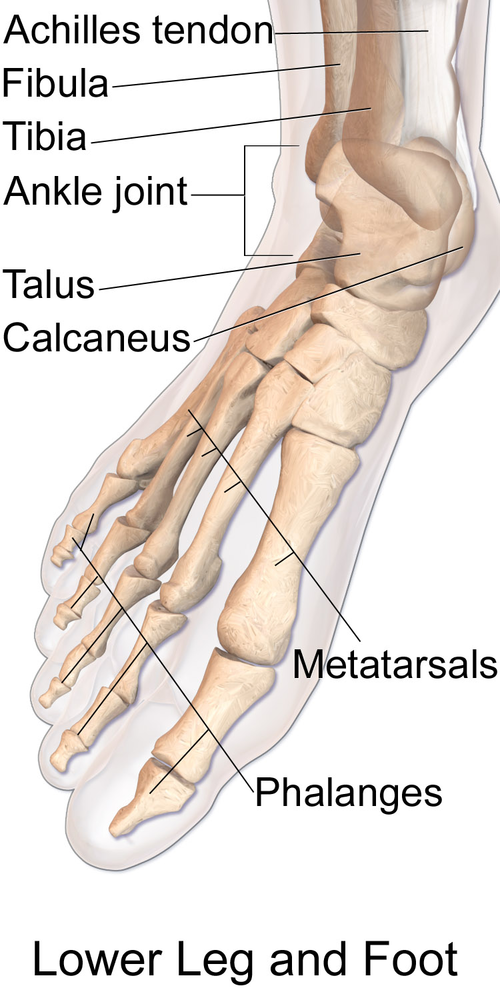
Foot and ankle region
The ankle/foot joint is composed of eight (8) articulations which include the talocrural, subtalar, talocalaneonavicular, calcaneocuboid, transverse tarsal, tarsometatarsal, metatarsophalangeal, and interphalangeal joint.
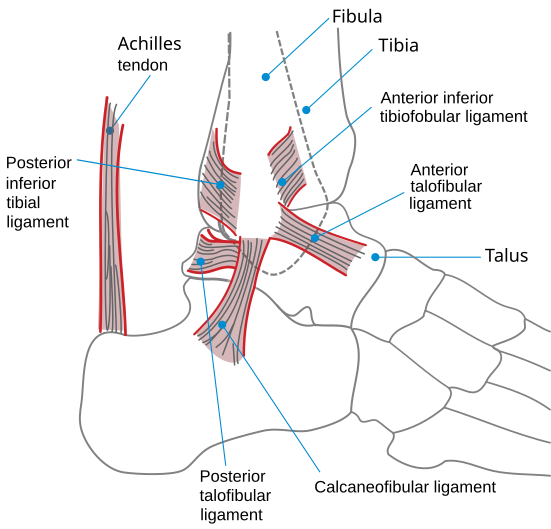
Ligaments of ankle
Bones of feet
The primary movements of the foot/ankle joint are:
Ankle plantarflexion/dorsiflexion
Ankle inversion/eversion
Other pertinent structures of the ankle/foot joint are:
Capsule
Provides stability to the joints of the ankle/foot
Ligaments
Talocrural joint
Medial collateral ligament- deep and superficial fibers
Lateral collateral ligament
Subtalar joint
Interosseous talocalcaneal ligament
Lateral talocalcaneal ligament
Posterior talocalcaneal ligament
Medial talocalcaneal ligament
Talonavicular joint
Plantar calcaneonavicular ligament
Dorsal talonavicular ligament
Calcaneocuboid joint
Medial band of bifurcate ligament
Medial calcaneocuboid
Long plantar ligament
Plantar calcaneocuboid
Tarsometatarsal joint
Medial dorsal ligament
Lateral dorsal ligament
Cuneonavicular joint
Plantar ligaments
Three (3) dorsal cuneonavicular ligaments
Metatarsophalangeal joint
Plantar ligaments
collateral ligaments
Interphalangeal joint
Plantar ligament
Collateral ligament
Plantar fascia
Collagen fibers connecting from medial calcaneus to phalanges
Fascia tightens during dorsiflexion- leads to supination and inversion
Bursa - act as fluid-filled sac that provides cushioning and friction reduction between tendons, joints, muscles and bone
Lower extremity range of motion normals
Lower extremity special tests
Hip special test
Hip scour test
Patient supine with hip flexed and adducted to the limit of movement; add compressive load
Tests for general hip pathology and degenerative joint disease
Positive: reproduction of pain symptoms or apprehension to perform
Patrick (FABIR) test
Patient supine, passively flex, abduct, and externally rotate test leg so the foot is resting above knee on opposite leg; then slowly leg down toward the table
Identifiers dysfunction of hip, specifically mobility dysfunction
Positive: involved knee is unable to assume relaxed position and/or reproduction of painful symptoms
Thomas test
Patient supine; one hip and knee maximally flexed to chest with hold; opposite limb is kept straight on table
Tests for tightness of hip flexors
Positive: straight limb flexes and patient is unable to keep this leg straight on leg
Ober’s test
Patient side-lying; lower limb flexed at the hip and the knee; passively extend and abduct tested with knee in 90 degrees while slowly lower the limb toward the table
Tests for tightness of tensor fascia late or iliotibial band
Positive: uppermost leg remains above horizontal
Ely’s test
Patient is prone; flex knee of tested limb
Tests for tightness of rectus femoris
Positive: hip of tested limb flexes
90-90 hamstring test
Patient position in supine; hip and knee supported in 90 degrees flexion; passively extend knee until end feel encountered
Test for tightness of the hamstrings
Positive: knee lacks 10 degrees or greater of knee extension
Piriformis test
Patient supine with foot tested limb passively placed lateral to opposite limb’s knee with tested adducted
Tests for piriformis tightness and syndrome
Positive: tested knee is unable to pass over resting knee or reproduction of pain- pain in buttocks or sciatic nerve pain
Trendelenburg test
Patient standing and asked to stand on one leg; observe for stance leg pelvis
Tests for gluteus medius weakness
Positive: stance pelvis drops when in single leg stance
Knee special test
Lachman test
Patient supine with knee flexed to 20-30 degrees; stabilize the femur and passively translate tibia anteriorly
Tests the integrity of the anterior cruciate ligament
Positive: excessive anterior translation on tibia compared to uninvolved limb
Test has higher sensitivity and specificity compared to anterior drawer test (preferred test)
Anterior drawer test
Patient supine with knee flexed to 45-90 degrees; therapist passively translates knee anteriorly
Tests the integrity of the anterior cruciate ligament
Positive: excessive anterior translation on tibia compared to uninvolved limb
Posterior drawer test
Patient in supine with knee flexed to 45 degrees; therapist passively translates tibia posteriorly
Tests integrity of posterior cruciate ligament
Positive: excessive posterior translation on tibia compared to uninvolved limb
Valgus stress test
Patient supine with knee resting at edge of mat; therapist applies valgus stress to the knee with knee flexed at 0 and 30 degrees
Tests the integrity of medial collateral ligament
Positive: laxity and pain compared to uninvolved side
Varus stress test
Patient supine with knee resting at edge of mat; therapist applies varus stress to knee with knee flexed at 0 and 30 degrees
Tests integrity of lateral collateral ligament
Positive: laxity and pain compared to uninvolved side
Pivot shift test
Patient supine with knee extended, hip flexed and abducted to 30 degrees and slight internal rotation; therapist holding knee with hand and the foot with another applies valgus force through a flexed knee
Tests the integrity of the anterior cruciate ligament
Positive: tibia reduction during the test by iliotibial band
McMurray test
Patient supine with knee maximally flexed; therapist passively internally rotates and extending knee- then moving to externally rotating and extending knee
Test lateral meniscus (internal rotation) and medial meniscus (external rotation)
Positive: reproduction of click, popping, or pain in knee
Apley’s Compression Test
Patient positioned prone with the knee flexed to 90 degrees.The therapist applies a downward compressive force through the heel while medially and laterally rotating the tibia.
Tests the integrity of menisci of the knee
Positive: reproduction of pain
Thessaly test
Patient standing on involved leg while holding therapist’s hands; patient rotates body and leg internally and externally with knee flexed to 5 degrees and then at 20 degrees
Test lateral meniscus (internal rotation) and medial meniscus (external rotation)
Positive: reproduction of click, popping, or pain in knee
Patellofemoral instability
Patient supine with knee flexed to 30 degrees and quadriceps are relaxed; therapist passively translates the patella laterally
Test for patellar instability
Positive: patient expresses apprehension or contracts the quadriceps muscle to prevent patellar dislocation.
Noble compression test
Patient supine with knee flexed to 90 degrees and hip flexion; therapist applies pressure 1-2cm proximal to lateral femoral epicondyle; with pressure maintaining, patient’s knee is passively extended
Tests the iliotibial band
Positive: patient experiences pain over the lateral femoral condyle
Ottwaa knee rules
Apply the Ottwa knee rules to:
Rule out fracture after acute knee injury
Refer for imaging with one or more positive answers
A negative test result states there is an absence of fracture
If therapist answers yes to any of these questions, then imaging should be done to rule out fracture
Age 55 years or older
Isolated patellar tenderness without bone tenderness
Tenderness of the fibula head
Inability to flex knee to 90 degrees
Inability to bear weight immediately after injury
Ankle special test
Anterior drawer test
Patient supine with foot off edge of mat; ankle in 20 degrees of plantarflexion; therapist translates talus anteriorly while stabilizing lower leg
Patient side-lying with knee slightly flexed and ankle in neutral position; therapist moves foot into maximal adduction (calceniofibular ligament) and abduction (deltoid ligament)
Tests the integrity of calcaneofibular ligament
Positive: laxity and/or pain
Thompson’s test
Patient prone with foot off edge of mat; therapists squeezes calf muscle (ankle should plantarflex)
Tests integrity of Achilles tendon
Positive: no movement of foot
Immediate red flag if positive tests occurs- send to emergency room
Windlass test
Weight bearing
Patient standing on step with toes positioned over the edge with equal weight baring; this causes a passive extension of the first MTP joint
Non-weight bearing
Patient seated with knee flexed to 90 degrees; therapist stabilizes the ankle and passively extends the patient’s first MTP joint
Both tests for the presence of plantar fasciitis
Positive in both positions: reproduction of plantar surface pain
Sign up for free to take 15 quiz questions on this topic