

















Special tests of lower extremity
Lower extremity special tests
Hip special test
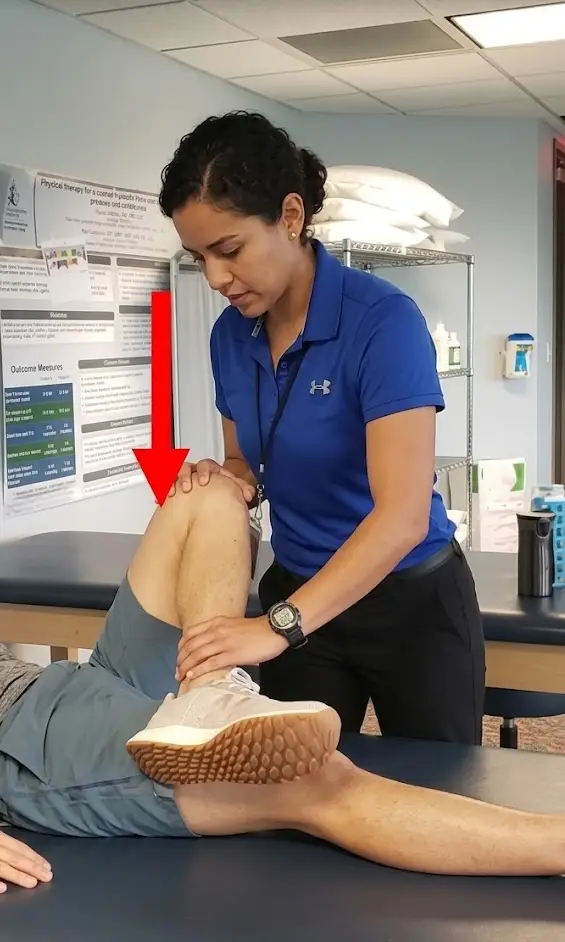
- Hip scour test
- Examiner applies downward pressure along the femoral shaft while repeatedly externally & internally rotating the hip with multiple angles of flexion.
- Tests for general hip pathology and degenerative joint disease
- Positive: reproduction of pain symptoms or apprehension to perform
- Examiner applies downward pressure along the femoral shaft while repeatedly externally & internally rotating the hip with multiple angles of flexion.
- Patrick (FABER) test
- Patient supine, passively flex, abduct, and externally rotate the test leg so the foot is resting above the knee on the opposite leg; then slowly leg toward the table
- Identifiers : dysfunction of the hip, specifically mobility dysfunction
- Positive: involved knee is unable to assume a relaxed position and/or reproduce painful symptoms
- Patient supine, passively flex, abduct, and externally rotate the test leg so the foot is resting above the knee on the opposite leg; then slowly leg toward the table
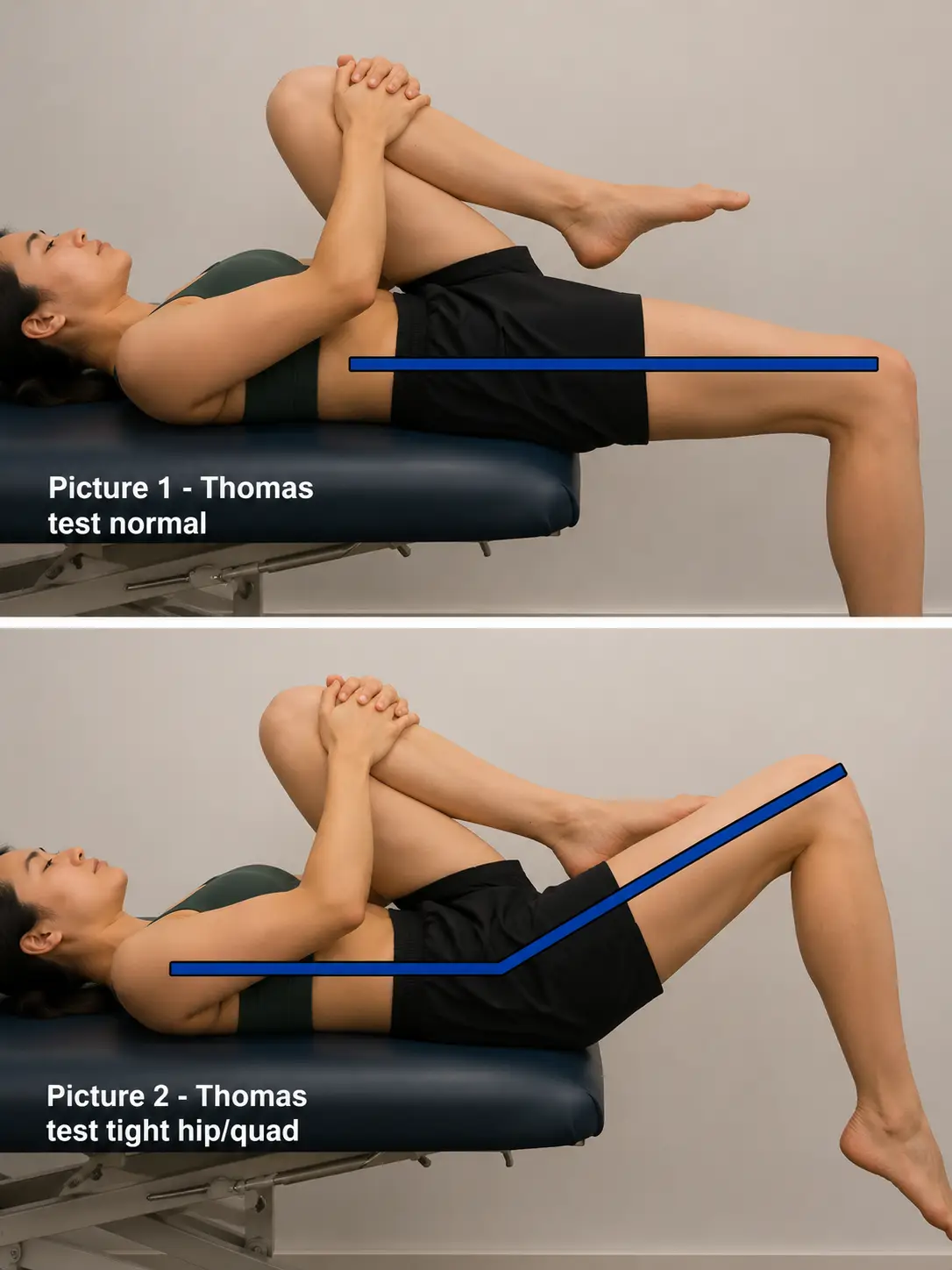
- Thomas test
- Patient supine; one hip and knee maximally flexed to the chest with hold; opposite limb is kept straight on the table
- Tests for the tightness of hip flexors
- Positive: straight limb flexes, and the patient is unable to keep this leg straight on the leg
- Patient supine; one hip and knee maximally flexed to the chest with hold; opposite limb is kept straight on the table
- Ober’s test
- Patient side-lying; lower limb flexed at the hip and the knee; passively extend and abduct tested with the knee at 90 degrees while slowly lowering the limb toward the table
- Tests for the tightness of the tensor fascia lata or the iliotibial band
- Positive: uppermost leg remains above horizontal
- Patient side-lying; lower limb flexed at the hip and the knee; passively extend and abduct tested with the knee at 90 degrees while slowly lowering the limb toward the table
- Ely’s test
- Patient is prone; flex the knee of the tested limb
- Tests for the tightness of the rectus femoris
- Positive: hip of the tested limb flexes
- Patient is prone; flex the knee of the tested limb
- 90-90 hamstring test
- Patient position in supine; hip and knee supported in 90 degrees flexion; passively extend the knee until end feel is encountered
- Test for the tightness of the hamstrings
- Positive: knee lacks 10 degrees or greater of knee extension
- Patient position in supine; hip and knee supported in 90 degrees flexion; passively extend the knee until end feel is encountered
- Piriformis test
- Patient lying with the foot tested limb passively placed lateral to the opposite limb’s knee, with the tested limb adducted
- Tests for piriformis tightness and syndrome
- Positive: tested knee is unable to pass over resting knee or reproduction of pain- pain in buttocks or sciatic nerve pain
- Patient lying with the foot tested limb passively placed lateral to the opposite limb’s knee, with the tested limb adducted
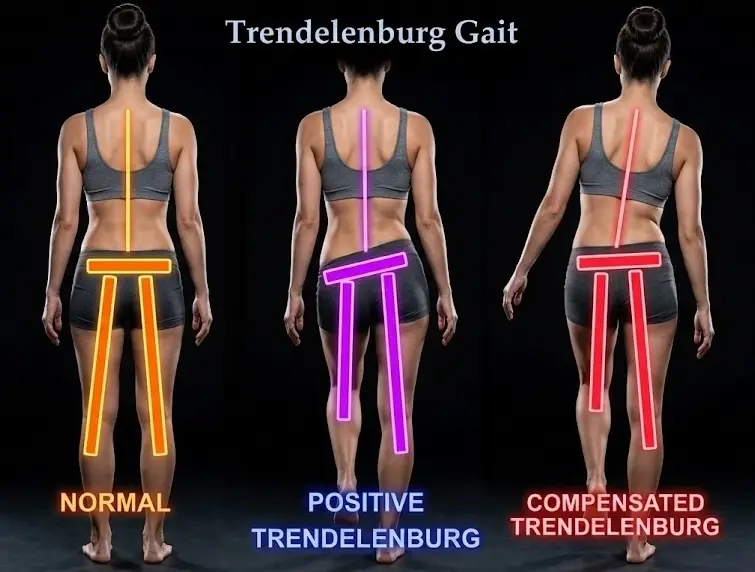
- Trendelenburg test
- Patient standing and asked to stand on one leg; observe the pelvis of the stance leg.
- Tests for gluteus medius weakness
- Positive: swing side pelvis drops when in single leg stance, or compensation by leaning the trunk over the stance leg
- Patient standing and asked to stand on one leg; observe the pelvis of the stance leg.
Knee special test
- Lachman test
- Patient supine with knee flexed to 20-30 degrees; stabilize the femur and passively translate the tibia anteriorly
- Tests the integrity of the anterior cruciate ligament
- Positive: excessive anterior translation on the tibia compared to the uninvolved limb
- Test has higher sensitivity and specificity compared to the anterior drawer test (preferred test)
- Patient supine with knee flexed to 20-30 degrees; stabilize the femur and passively translate the tibia anteriorly
- Anterior drawer test
- Patient supine with knee flexed to 45-90 degrees; therapist passively translates the knee anteriorly
- Tests the integrity of the anterior cruciate ligament
- Positive: excessive anterior translation on the tibia compared to the uninvolved limb
- Patient supine with knee flexed to 45-90 degrees; therapist passively translates the knee anteriorly
- Posterior drawer test
- Patient in supine with knee flexed to 45 degrees; therapist passively translates tibia posteriorly
- Tests the integrity of the posterior cruciate ligament
- Positive: excessive posterior translation on the tibia compared to the uninvolved limb
- Patient in supine with knee flexed to 45 degrees; therapist passively translates tibia posteriorly
-
Valgus stress test
- Patient supine with knee resting at the edge of the mat; therapist applies valgus stress to the knee with the knee flexed at 0 and 30 degrees
- Tests the integrity of the medial collateral ligament
- Positive: laxity and pain compared to the uninvolved side
- Patient supine with knee resting at the edge of the mat; therapist applies valgus stress to the knee with the knee flexed at 0 and 30 degrees
-
Varus stress test
- Patient supine with knee resting at the edge of the mat; therapist applies varus stress to the knee with the knee flexed at 0 and 30 degrees
- Tests the integrity of the lateral collateral ligament
- Positive: laxity and pain compared to the uninvolved side
- Patient supine with knee resting at the edge of the mat; therapist applies varus stress to the knee with the knee flexed at 0 and 30 degrees
- Pivot shift test
- Patient supine with knee extended, hip flexed, and abducted to 30 degrees and slight internal rotation; therapist holding knee with one hand and the foot with the other applies valgus force through a flexed knee
- Tests the integrity of the anterior cruciate ligament
- Positive: tibia reduction during the test by the iliotibial band
- Patient supine with knee extended, hip flexed, and abducted to 30 degrees and slight internal rotation; therapist holding knee with one hand and the foot with the other applies valgus force through a flexed knee
- McMurray test
- Patient supine with knee maximally flexed; therapist passively internally rotates and extends the knee,- then moves to externally rotating and extending the knee
- Test the lateral meniscus (internal rotation) and the medial meniscus (external rotation)
- Positive: reproduction of click, popping, or pain in the knee
- Patient supine with knee maximally flexed; therapist passively internally rotates and extends the knee,- then moves to externally rotating and extending the knee
- Apley’s Compression test
- Patient positioned prone with the knee flexed to 90 degrees. The therapist applies a downward compressive force through the heel while medially and laterally rotating the tibia.
- Tests the integrity of the menisci of the knee
- Positive: reproduction of pain
- Patient positioned prone with the knee flexed to 90 degrees. The therapist applies a downward compressive force through the heel while medially and laterally rotating the tibia.
- Thessaly test
- Patient standing on involved leg while holding therapist’s hands; patient rotates body and leg internally and externally with knee flexed to 5 degrees and then at 20 degrees
- Test the lateral meniscus (internal rotation) and the medial meniscus (external rotation)
- Positive: reproduction of click, popping, or pain in the knee
- Patient standing on involved leg while holding therapist’s hands; patient rotates body and leg internally and externally with knee flexed to 5 degrees and then at 20 degrees
-
Patellofemoral instability
- Patient supine with knee flexed to 30 degrees and quadriceps relaxed; therapist passively translates the patella laterally
- Test for patellar instability
- Positive: patient expresses apprehension or contracts the quadriceps muscle to prevent patellar dislocation
- Patient supine with knee flexed to 30 degrees and quadriceps relaxed; therapist passively translates the patella laterally
-
Noble compression test
- Patient supine with knee flexed to 90 degrees and hip flexion; therapist applies pressure 1-2cm proximal to the lateral femoral epicondyle; with pressure maintained, the patient’s knee is passively extended
- Tests the iliotibial band
- Positive: patient experiences pain over the lateral femoral condyle
- Patient supine with knee flexed to 90 degrees and hip flexion; therapist applies pressure 1-2cm proximal to the lateral femoral epicondyle; with pressure maintained, the patient’s knee is passively extended
- Ottawa knee rules
- Apply the Ottawa knee rules to:
- Rule out fracture after acute knee injury
- Refer for imaging with one or more positive answers
- A negative test result states there is an absence of fracture
- If the therapist answers yes to any of these questions, then imaging should be done to rule out a fracture
- Age 55 years or older
- Isolated patellar tenderness without bone tenderness
- Tenderness of the fibula head
- Inability to actively flex knee to 90 degrees
- Inability to bear weight immediately after injury
- Apply the Ottawa knee rules to:
Ankle special test
-
Anterior drawer test
- Patient supine with foot off the edge of the mat; ankle in 20 degrees of plantarflexion; therapist translates the talus anteriorly while stabilizing the lower leg
- Tests the integrity of the anterior talofibular ligament
- Positive: excessive anterior talar translation and/or pain
- Patient supine with foot off the edge of the mat; ankle in 20 degrees of plantarflexion; therapist translates the talus anteriorly while stabilizing the lower leg
-
Talar tilt
- Position: Patient sits with the knee bent and the ankle hanging free (neutral to 10-20 degrees plantar flexion).
- Stabilization: The clinician stabilizes the distal tibia (lower leg) with one hand.
- Therapist moves foot into maximal adduction (calcaneofibular ligament) and abduction (deltoid ligament)
- Tests the integrity of the calcaneofibular ligament
- Positive: laxity and/or pain
- Thompson’s test
- Patient prone with foot off the edge of the mat; therapists squeeze calf muscle (ankle should plantarflex)
- Tests the integrity of the Achilles tendon
- Positive: no movement of the foot
- Immediate red flag if positive tests occur- send to emergency room
- Patient prone with foot off the edge of the mat; therapists squeeze calf muscle (ankle should plantarflex)
- Windlass test
-
Weight bearing
- Patient standing on the step with toes positioned over the edge with equal weight bearing; this causes a passive extension of the first MTP joint
- Procedure: The examiner passively dorsiflexes (bends upwards) the first metatarsophalangeal (MTP) joint, or big toe, while keeping the interphalangeal joint relaxed
-
Non-weight bearing
- Patient seated with knee flexed to 90 degrees; therapist stabilizes the ankle and passively extends the patient’s first MTP joint
- Both tests for the presence of plantar fasciitis
- Patient seated with knee flexed to 90 degrees; therapist stabilizes the ankle and passively extends the patient’s first MTP joint
-
Positive in both positions: reproduction of plantar surface pain, or the joint does not extend
-