
























Special tests of upper extremity
Shoulder special tests
- Apprehension test (tests anterior instability)
- Patient is supine, the shoulder is in 90 degrees of abduction; therapist attempts to externally rotate
- Positive: patient seems apprehensive about performing movement and resists motion
- Patient is supine, the shoulder is in 90 degrees of abduction; therapist attempts to externally rotate
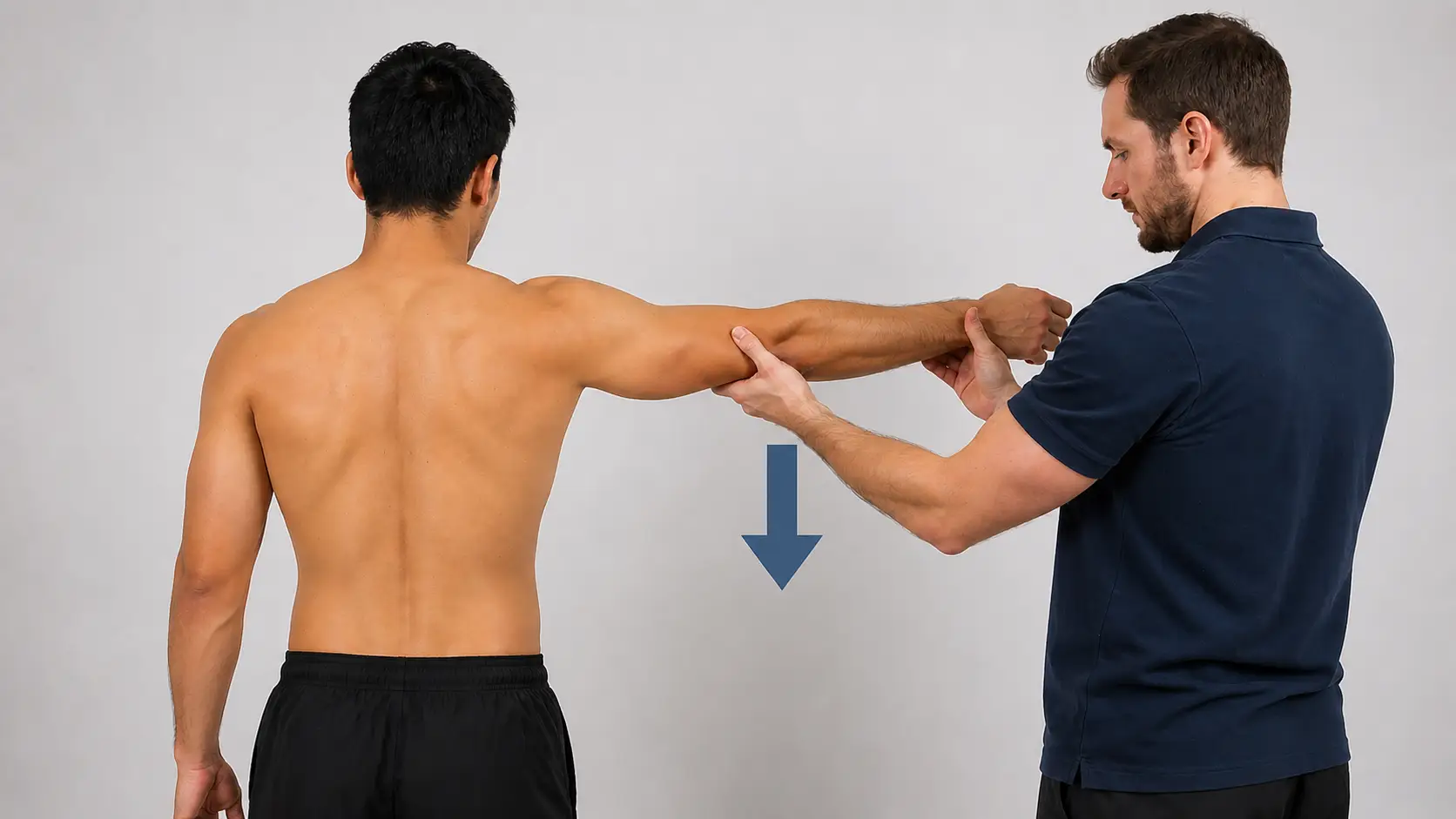
- Sulcus sign (tests posterior and inferior instability)
- Patient stands with arm relaxed at the side; therapist pulls the arm distally
- Positive: presence of sulcus inferior to the acromion with symptom reproduction
- Patient stands with arm relaxed at the side; therapist pulls the arm distally
- Drop arm test
- Patient seated with the shoulder passively abducted to 90 degrees and externally rotated; patient instructed to slowly lower the arm back to the side
- Positive: patient is unable to lower their arm down slowly and suddenly drops to the side without control
- Patient seated with the shoulder passively abducted to 90 degrees and externally rotated; patient instructed to slowly lower the arm back to the side
- Infraspinatus/supraspinatus muscle test
- Patient is seated, or standing, and therapist resists external rotation with the arm in the neutral position and adducted to the trunk
- Positive: patient is unable to sustain external rotation
- Patient is seated, or standing, and therapist resists external rotation with the arm in the neutral position and adducted to the trunk
- External rotation lag sign
- Patient is seated or standing with the shoulder passively abducted to 90 degrees and externally rotated
- Positive: patient is unable to maintain external rotation
- Patient is seated or standing with the shoulder passively abducted to 90 degrees and externally rotated
- Lift off test (Gerber’s test)
- Patient is standing with the shoulder passively placed in internal rotation and the hand at waist level against the back
- Positive: patient is unable to lift off the back
- Patient is standing with the shoulder passively placed in internal rotation and the hand at waist level against the back
- Internal rotation lag sign
- Patient is seated with arm held behind the back in internal rotation passively
- Positive: patient is unable to maintain internal rotation
- Patient is seated with arm held behind the back in internal rotation passively
- Empty can test
- The patient stands or sits with their arms at their sides. The patient abducts their arm to 90 degrees, with their elbow extended. The patient internally rotates their shoulders so that their thumbs point towards the floor. The examiner applies downward pressure on the patient’s wrist or forearm.
- Positive: Pain in the shoulder, weakness in the arm, and the patient’s arm dropping involuntarily.
- Tests the supraspinatus muscle
- Positive: Pain in the shoulder, weakness in the arm, and the patient’s arm dropping involuntarily.
- The patient stands or sits with their arms at their sides. The patient abducts their arm to 90 degrees, with their elbow extended. The patient internally rotates their shoulders so that their thumbs point towards the floor. The examiner applies downward pressure on the patient’s wrist or forearm.
- Neer’s
- The patient sits comfortably, and the examiner stands behind them. The examiner stabilizes the patient’s scapula (shoulder blade) with one hand to prevent scapular movement during the test. The examiner passively flexes the patient’s arm forward while internally rotating it, bringing the greater tuberosity of the humerus (the bony bump on the upper arm) under the acromion.
- Positive: The patient reports pain or tenderness during arm movement, particularly in the anterior or lateral aspect of the shoulder.
- Tests for impingement
- Positive: The patient reports pain or tenderness during arm movement, particularly in the anterior or lateral aspect of the shoulder.
- The patient sits comfortably, and the examiner stands behind them. The examiner stabilizes the patient’s scapula (shoulder blade) with one hand to prevent scapular movement during the test. The examiner passively flexes the patient’s arm forward while internally rotating it, bringing the greater tuberosity of the humerus (the bony bump on the upper arm) under the acromion.
- Hawkins-Kennedy
- The patient sits with their arm flexed at the shoulder and elbow to 90 degrees. The examiner stabilizes the patient’s shoulder with one hand and internally rotates the arm with the other hand.
- Positive: The test is considered positive if the patient experiences pain in the anterior shoulder during internal rotation.
- Tests for impingement
- Positive: The test is considered positive if the patient experiences pain in the anterior shoulder during internal rotation.
- The patient sits with their arm flexed at the shoulder and elbow to 90 degrees. The examiner stabilizes the patient’s shoulder with one hand and internally rotates the arm with the other hand.
- Acromioclavicular (AC) joint
- Horizontal adduction test
- Patient standing with shoulder flexed to 90 degrees and adducted across the chest
- Positive: localized pain over the AC joint
- Patient standing with shoulder flexed to 90 degrees and adducted across the chest
- Horizontal adduction test
- SLAP (superior labrum anterior to posterior) lesions
- O’Brien’s test
- The patient stands or sits with their affected arm flexed at 90° and adducted 10–15°; the patient internally rotates their shoulder; the examiner applies downward pressure on the patient’s arm while the patient resists; repeated with the upper extremity in external rotation
- Positive: pain or clicking noise found when performing internal rotation and symptoms relieved when performing external rotation
- Differential diagnosis needs to be made to determine if AC joint vs glenohumeral joint dysfunction
- The patient stands or sits with their affected arm flexed at 90° and adducted 10–15°; the patient internally rotates their shoulder; the examiner applies downward pressure on the patient’s arm while the patient resists; repeated with the upper extremity in external rotation
- O’Brien’s test
- Bicep tendonitis tests
- Bicep load II test
- Patient in supine with shoulder abducted to 120 degrees, elbow flexed to 90 degrees, forearm supinated; shoulder fully externally rotated; if the patient demonstrates apprehension when performing, then asked to flex the elbow against resistance
- Positive: if apprehension remains the same or the shoulder becomes more painful
- Patient in supine with shoulder abducted to 120 degrees, elbow flexed to 90 degrees, forearm supinated; shoulder fully externally rotated; if the patient demonstrates apprehension when performing, then asked to flex the elbow against resistance
- Bicep load II test
- Yergason’s test
- Patient sitting with shoulder in neutral position against trunk, elbow at 90 degrees, and forearm pronated, resist supination of forearm and external rotation of shoulder
- Tests for transverse ligament, bicipital tendonitis, and SLAP lesions
- Positive: biceps tendon of long head will be palpable outside of the bicipital groove, or a reproduction of pain
- Patient sitting with shoulder in neutral position against trunk, elbow at 90 degrees, and forearm pronated, resist supination of forearm and external rotation of shoulder
- Speed’s test
- Patient sitting or standing with upper limb in full extension (at the side) and forearm supination, resist shoulder flexion
- Can also place the shoulder in 90 degrees of flexion and push the upper limb into extension (causing eccentric contraction)
- Tests bicipital tendonitis and SLAP lesions
- Positive: pain in bicipital groove at the anterior shoulder
Elbow special tests
- Elbow extension test
- Patient in seated position attempts to fully extend the elbow
- Positive: patient unable to extend due to possible fracture — imaging will be needed to confirm
- Varus/valgus test
- Patient sitting or supine with elbow flexed to 20 degrees; valgus force applied to test the ulnar collateral ligament, and then varus force applied to test for the radial collateral ligament
- Positive: joint laxity and possible pain- needs to be performed bilaterally to determine joint laxity
- Bicep squeeze test for bicep rupture sign
- Observation of distal bunching of the bicep muscle along with complete loss of function (unable to perform elbow flexion)
- Positive: Indicates rupture of the proximal long head of the biceps tendon
- Cozen’s test
- Patient can be seated or standing. Position the patient with their elbow extended, forearm in pronation, wrist in slight radial deviation, and then ask them to make a fist and resist wrist extension while the examiner palpates the lateral epicondyle.
- Positive: Pain indicates lateral epicondylitis
- Mills test
- The patient is seated, and the clinician palpates the patient’s lateral epicondyle with one hand while pronating the patient’s forearm, fully flexing the wrist, the elbow extended
- Positive: Pain with this maneuver suggests lateral epicondylitis.
- The patient is seated, and the clinician palpates the patient’s lateral epicondyle with one hand while pronating the patient’s forearm, fully flexing the wrist, the elbow extended
-
Reverse Mills test
-
The patient can be seated or standing. The clinician stabilizes the patient’s humerus, palpates the medial epicondyle, and then passively supinates the patient’s forearm, extends the wrist, and fully extends the elbow causing a stretch in the flexor tendons.
-
Positive: Pain with this maneuver suggests medial epicondylitis
-
Medial epicondylitis (Golfer’s elbow) test
- The patient is seated, and the clinician palpates the patient’s medial epicondyle with one hand while extension the elbow and fully extending the wrist.
- Positive: Pain with this maneuver suggests medial epicondylitis.
-
-
Neurological dysfunction
- Elbow flexion test (Wadsworth Test)
- Patient supine with shoulder in full external rotation and elbow held in maximal flexion with wrist extended for one minute
- Positive: pain present at the medial elbow within the ulnar distribution of the involved side
- Entrapment of the ulnar nerve at the cubital tunnel
- Elbow flexion test (Wadsworth Test)
- Varus/valgus test
- Patient sitting or supine with elbow flexed to 20 degrees; valgus force applied to test ulnar collateral ligament (UCL) and then varus force applied to test for radial collateral ligament (RCL)
- Positive; joint laxity and possible pain- needs to be performed bilaterally to determine joint laxity
- Patient sitting or supine with elbow flexed to 20 degrees; valgus force applied to test ulnar collateral ligament (UCL) and then varus force applied to test for radial collateral ligament (RCL)
Wrist and hand special tests
Ligamentous, capsule, and joint instability
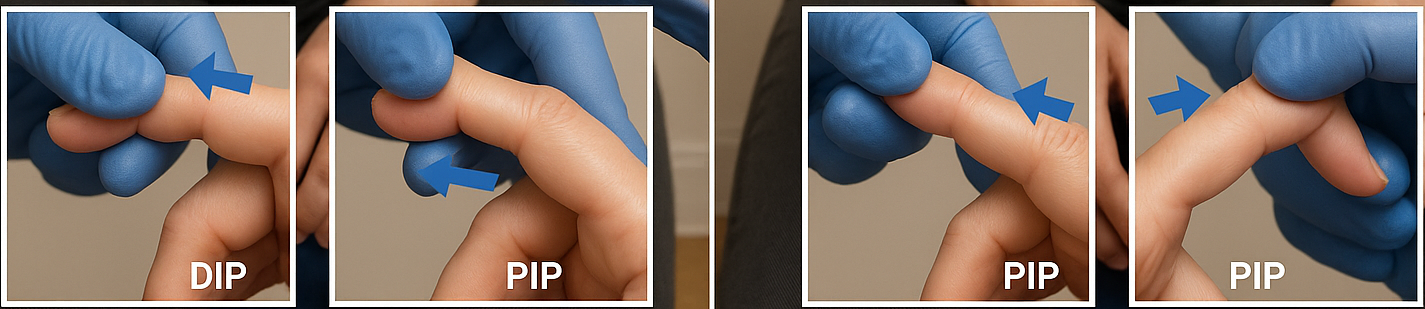
- Interphalangeal joint varus/valgus tests
- Patient in a seated position with fingers supported and stabilized; valgus/varus force applied to PIP and DIP joints of all digits
- Positive: joint laxity and possible pain - needs to be performed bilaterally to determine the extent of laxity
Tendon and muscle
Finkelstein’s test and Eichhoff’s test are traditional provocative tests for de Quervain’s tenosynovitis. The WHAT (Wrist Hyperflexion Abduction of the Thumb) test has shown a very high sensitivity (99%) but low specificity.
- Wrist hyperabduction and abduction of thumb test (WHAT)
- Patient in seated position with wrist hyperflexed and thumb abducted in full MCP and IP extension. The examiner applies a gradually increasing abduction resistance to the thumb,
- Positive: reproduction of pain in wrist- needs to be performed bilaterally
- Indicates de Quervain’s tenosynovitis in the 1st dorsal compartment (abductor pollicis longus and extensor pollicis brevis.
- Eichoff’s test
- Eichoff’s test
- Patient seated makes fist with thumb flexed within fingers while the patient actively moves wrist into ulnar deviation
- Positive: reproduction of pain in wrist- needs to be performed bilaterally
- Indicates de Quervain’s tenosynovitis in the 1st dorsal compartment (abductor pollicis longus and extensor pollicis braves
- Eichoff’s test
- Finkelstein’s test
- Patient seated makes fist with thumb flexed within fingers while examiner passively moves wrist into ulnar deviation
- Positive: reproduction of pain in wrist- needs to be performed bilaterally
- Indicates de Quervain’s tenosynovitis in the 1st dorsal compartment (abductor pollicis longus and extensor pollicis brevis
- Patient seated makes fist with thumb flexed within fingers while examiner passively moves wrist into ulnar deviation
Neurological dysfunction
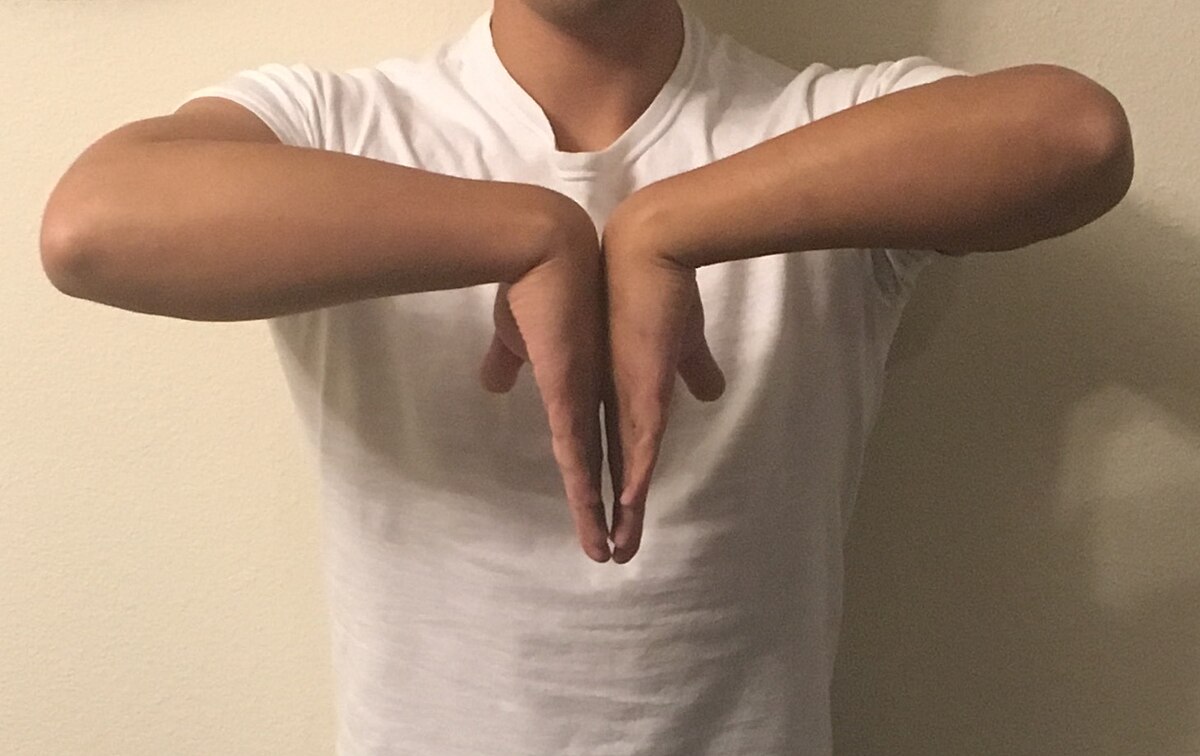
- Phalen’s test (wrist flexion test)
- Patient in seated position maximally flexes both wrists while holding them together for one minute
- Positive: reproduces tingling sensation or paresthesia in the median nerve distribution
- Indicates carpal tunnel syndrome
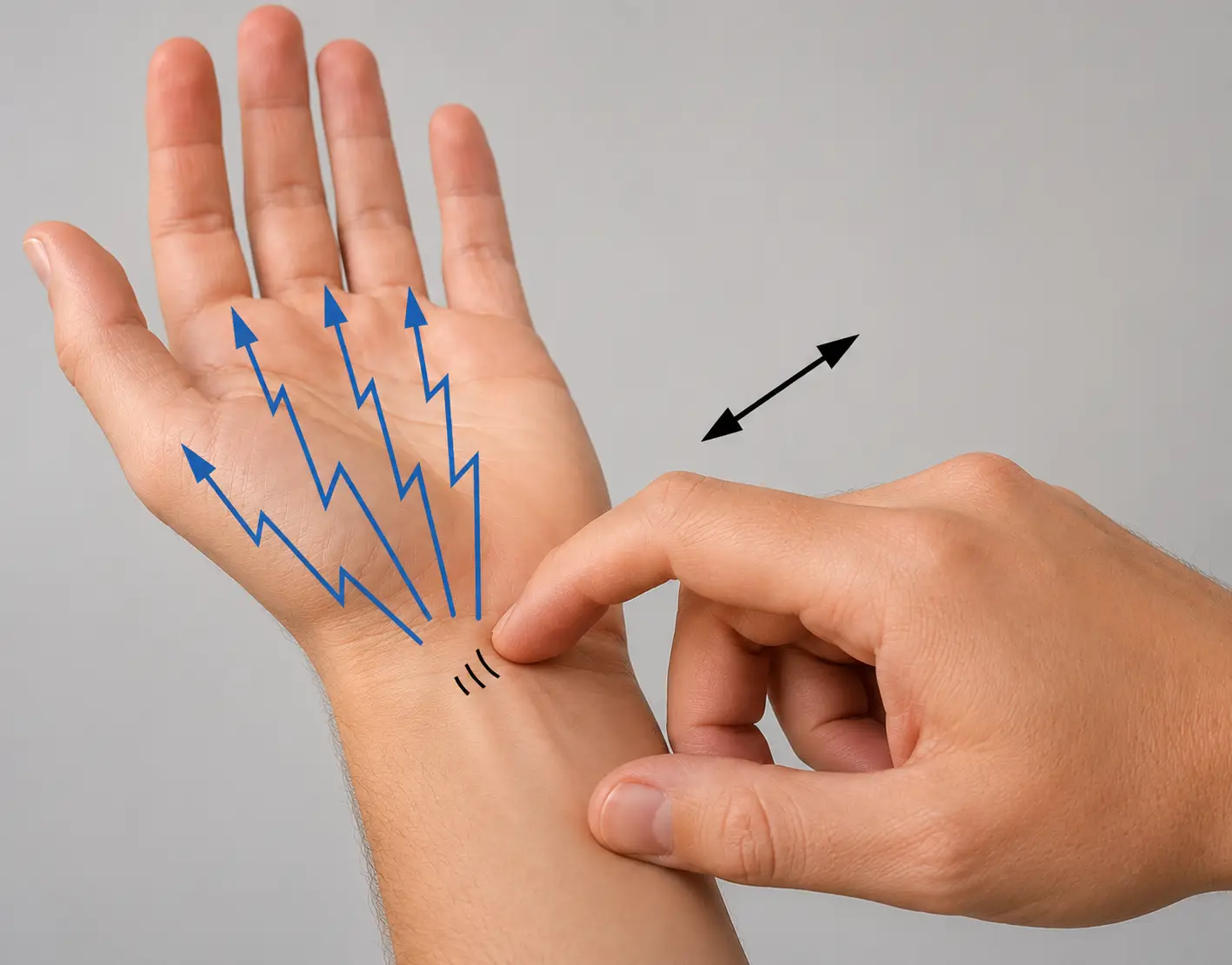
- Tinel’s test
- Patient in seated position, and the therapist taps the peripheral nerve (can be any nerve palpable)
- Positive: reproduces tingling sensation or paresthesia in the nerve distribution
Vascular dysfunction
- Modified Allen’s test
- Patient in seated position has therapist palpate the radial and ulnar nerve, followed by the patient quickly opening and closing their hand several times; the patient then makes a fist
- The therapist then compresses the radial artery, has the patient open the hand, observes the palm, releases the compressed radial artery, and observes for radial filling time; the same procedure will be done with the ulnar artery
- Positive: abnormal refilling time — needs to be performed bilaterally