


Taenia
Taenia
Also called tapeworms (cestodes), three species commonly cause human infection:
- Taenia saginata (beef tapeworm)
- Taenia solium (pork tapeworm)
- Taenia asiatica (Asian tapeworm)
You acquire intestinal taeniasis by eating raw or undercooked beef or pork containing larval cysts. In the USA, T. solium is more common and is often seen in Latin American immigrants.
Pathogenesis: Humans ingest Taenia in the cysticercus (larval) stage. In the intestine, the larva develops into an adult tapeworm, which may grow several meters long. Adult worms produce proglottids (egg-containing segments). These proglottids mature, become gravid, detach from the worm, and either migrate to the anus or are passed in stool. Eggs are released from proglottids and then infect cattle or pigs.
Clinical features: Most people are asymptomatic. When symptoms occur, tapeworms can cause digestive complaints such as abdominal pain, loss of appetite, weight loss, and upset stomach. The most visible sign of taeniasis is active passage of proglottids (tapeworm segments) through the anus and in the feces. Rarely, segments lodge in the appendix or in the bile or pancreatic ducts, causing obstructive symptoms. T. solium (NOT T. saginata) can cause cysticercosis.
Cysticercosis: Caused by ingestion of T. solium eggs. (This is different from intestinal taeniasis, which is acquired by ingesting cysticerci in undercooked pork or beef.) People do not get cysticercosis by eating undercooked pork. After egg ingestion, larvae develop into cysts that can infect the brain (neurocysticercosis), muscle, eyes, or other tissues. Symptoms depend on cyst location. Neurocysticercosis can present with seizures, headaches, confusion, stroke, etc. Muscle involvement may present as tender subcutaneous lumps.
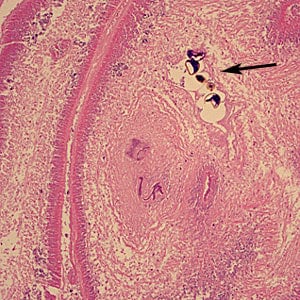
Section of human brain tissue with a cysticercus (H&E stained). The scolex (arrow) and bladder wall (darts) are indicated.
Diagnosis of Taeniasis: Laboratory diagnosis is made by demonstrating tapeworm eggs in stool samples. There may also be a history of passing tapeworm segments in stool. Antigen detection can be done by ELISA, while antibody detection can be done by ELISA, indirect haemagglutination, and indirect immunofluorescence. PCR and DNA probes can be used for molecular diagnosis.
Neurocysticercosis is diagnosed by ELISA and CSF immunoblot for antibodies, as well as antigen detection in CSF by ELISA. Tissue biopsy shows cysticerci. CT scan and MRI may show solitary or multiple calcified intracranial lesions/cysts.
Unstained Taenia sp. egg, teased from a proglottid of an adult. Four hooks can easily be seen in this image.
Diphyllobothrium latum
Diphyllobothrium latum is the largest tapeworm that infects humans and is associated with fish (the fish tapeworm). Infection is acquired by ingesting raw or undercooked fish. The parasite is killed by freezing and cooking.
Most infections are asymptomatic. When symptomatic, it may cause intestinal obstruction and gallbladder disease due to migration of proglottids. Vitamin B12 deficiency may occur. Diagnosis is made by identifying eggs and tapeworm segments in stool samples.
Sections of diphyllobothriid gravid proglottids containing eggs (arrow) in intestinal tissue, stained with H&E.
Echinococcus
Echinococcus is associated with unilocular or multilocular cysts in visceral organs. The cyst contains clear fluid, numerous brood capsules, and protoscolices. Protoscolices may settle at the bottom of the cyst, forming hydatid sand.
This tapeworm requires two hosts to complete its life cycle, mainly dogs and sheep.
- Infection with the larval stage of E. granulosus causes cystic echinococcosis.
- Infection with the larval stage of E. multilocularis causes alveolar echinococcosis.
Human infection occurs by ingesting food or water contaminated with tapeworm eggs. People who raise sheep are at high risk.
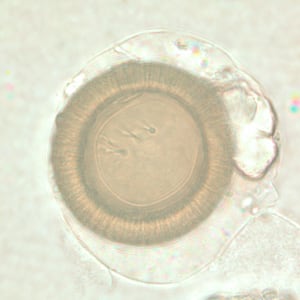
Close-up of the scolex of E. granulosus. In this focal plane, one of the suckers is clearly visible, as is the ring of rostellar hooks.
Echinococcus granulosus infections often remain asymptomatic for years, until cysts become large enough to cause symptoms in the affected organ. Hydatid cysts can develop in the liver, lungs, spleen, kidneys, CNS, etc. Rupture of a cyst can trigger a host reaction with fever, urticaria, eosinophilia, and anaphylactic shock. Rupture can also lead to dissemination of cyst contents.
A cyst-like mass in a person with exposure to sheep or dogs in an area where E. granulosus is endemic suggests cystic echinococcosis. Imaging (CT scan, ultrasonography, MRI) is used to detect cysts. After a cyst is detected, serologic tests can help confirm the diagnosis. Remember: stool examination is not the diagnostic test for echinococcosis.
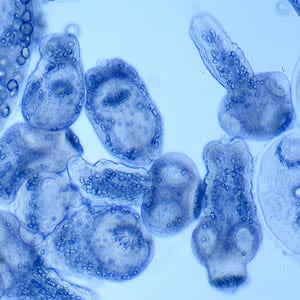
Protoscolices liberated from a hydatid cyst. The two protoscolices on the right side of the image are evaginated.
Cross-section of an E. granulosus cyst, stained with H&E. Host tissue (A) encapsulates the hydatid cyst wall, which is composed of an acellular laminated layer (B) and a nucleate germinal layer © from which the brood capsule (D) arises. Inside the brood capsule are numerous protoscolices (E) with visible hooklets (F).
Echinococcus multilocularis affects the liver as a slow-growing, destructive tumor. Early infection may present only with abdominal pain and biliary obstruction, and it may be misdiagnosed as liver cancer. Rarely, metastatic lesions occur in the lungs, spleen, and brain. Untreated infection has a high fatality rate. Alveolar echinococcosis is typically found in older people. Imaging (such as CT scans) is used to visually confirm parasitic vesicles and cyst-like structures, and serologic tests can confirm infection.