Spinal cord tracts and lesions
Corticospinal tract
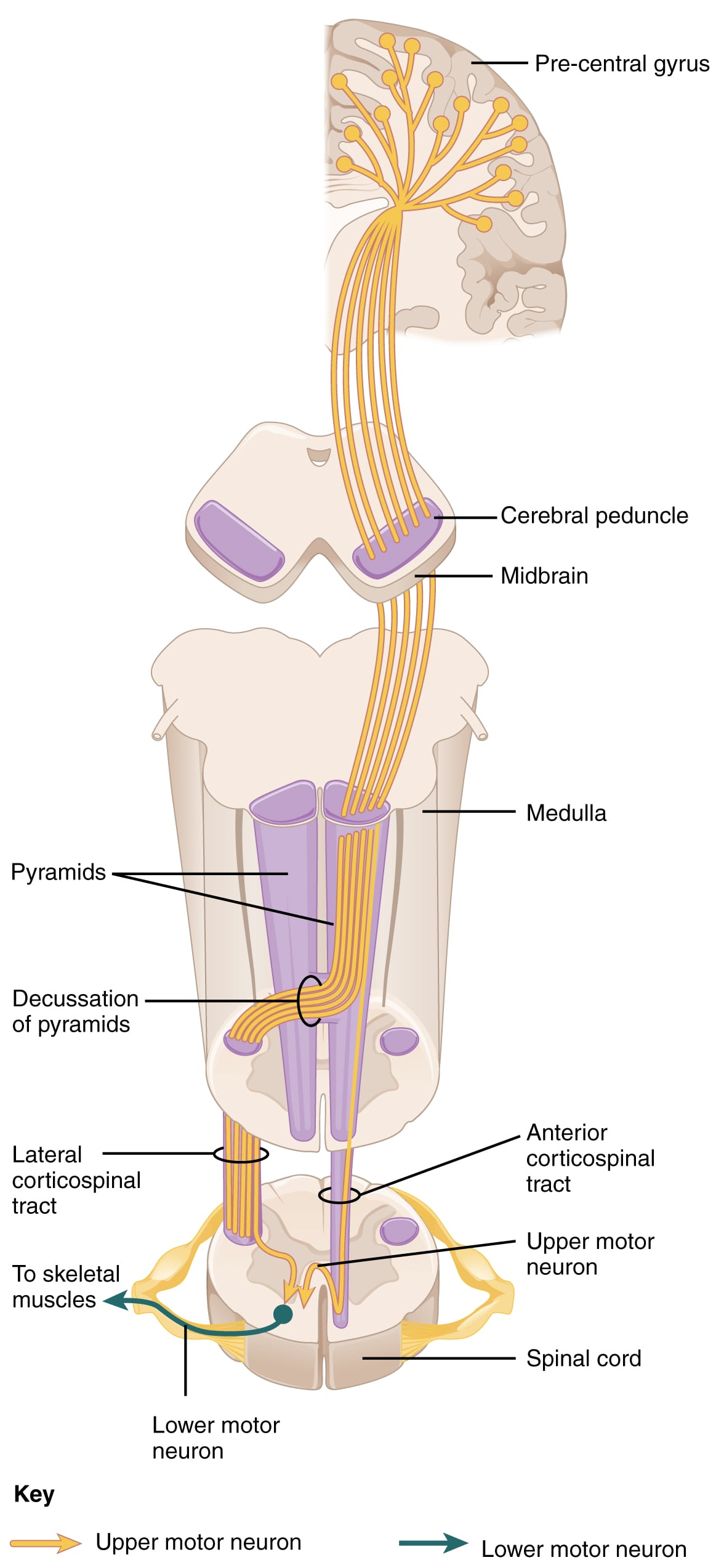
The corticospinal tract is a descending motor pathway that arises mostly from the primary motor cortex and premotor cortex (Brodman areas 4 and 6). Some fibers also arise from the primary and secondary somatosensory areas. These fibers pass through the internal capsule and descend ventrally through the midbrain, pons, and medulla.
In the lower medulla, about 85% to 90% of the fibers cross (decussate) at the pyramidal decussation to form the lateral corticospinal tract. These fibers continue descending in the lateral funiculus and terminate at all spinal cord levels.
At the pyramidal decussation, the remaining 10% to 15% of fibers do not cross. They descend uncrossed as the anterior corticospinal tract. These fibers primarily control proximal muscles, such as those of the trunk.
Lesion location determines the side of motor deficits:
- Lesions above the decussation cause contralateral symptoms.
- Lesions below the decussation (typically in the spinal cord) cause ipsilateral symptoms.
The primary function of the corticospinal tract is voluntary motor control of the body and limbs.
Rubrospinal, vestibulospinal and lateral and medial reticulospinal tracts
- The rubrospinal tract arises from the red nucleus of the midbrain and is associated with voluntary movement, especially flexor muscles of the upper limb.
- The lateral reticulospinal tract arises from the reticular formation in the medulla and inhibits spinal motor neurons.
- The medial reticulospinal tract arises from the pontine reticular formation and activates posture-related extensor muscles.
- The vestibulospinal tract activates posture-related extensor muscles.
Lissauer’s tract or dorsolateral tract of Lissauer
Lissauer’s tract is formed by the proximal ends of small unmyelinated and poorly myelinated fibers in peripheral nerves. These fibers enter at the lateral aspect of the dorsal horn, then ascend and descend up to four spinal cord segments before terminating in laminae I through VI of the ipsilateral dorsal horn. These axons mostly carry crude touch and pressure information. These fibers are closely related to the substantia gelatinosa.
Spinothalamic tract
The spinothalamic tract is an ascending sensory pathway that carries pain, temperature, crude touch, pressure, and nociception. It is divided into:
- The anterior spinothalamic tract (crude touch)
- The lateral spinothalamic tract (pain and temperature)
Pathway overview:
- The first-order neuron is a pseudounipolar neuron in the dorsal root ganglion.
- Its efferents travel in Lissauer’s tract and synapse on second-order neurons in the substantia gelatinosa (in the gray matter of the spinal cord).
- Axons from second-order neurons cross to the opposite side in the anterior commissure, typically two segments above the level of entry (remember this for the clinical presentation of syringomyelia).
- These fibers then ascend anterolaterally in the spinal cord and enter the brainstem as the spinal lemniscus.
- The tract terminates in the ventral posterolateral nucleus (VPL) of the thalamus, which contains the third-order neurons.
- Third-order axons ascend through the posterior limb of the internal capsule and terminate in the primary somatosensory area.
Somatotopy:
- Cervical areas are represented medially.
- Sacral areas are represented laterally.
Dorsal columns
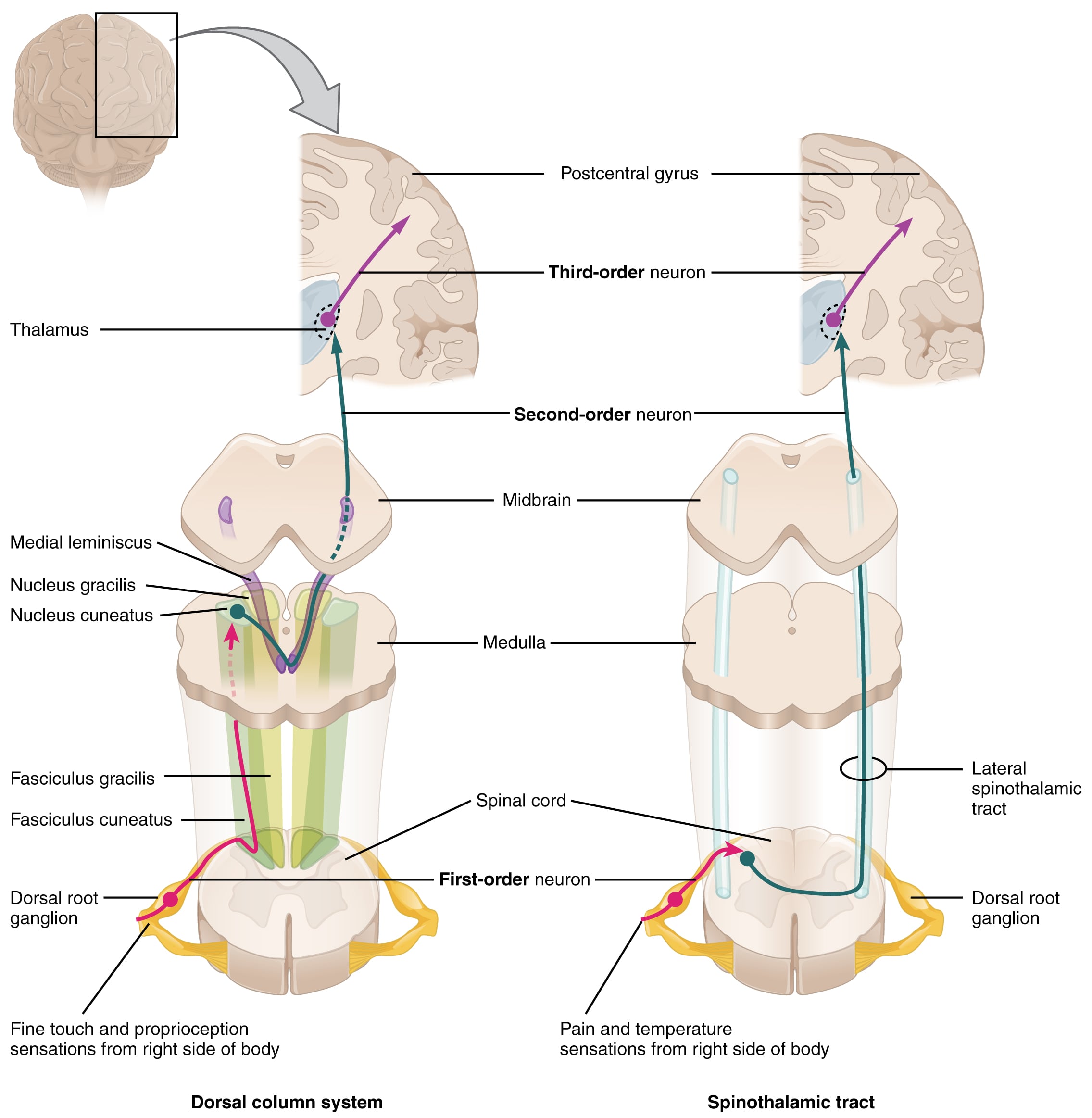
The dorsal columns are an ascending pathway that carries fine touch, two-point discrimination, proprioception, and vibration. This pathway is also called the dorsal column-medial lemniscus pathway.
Pathway overview:
- The first-order neuron is located in the dorsal root ganglion.
- It receives afferents from Meissner’s corpuscles, free nerve endings on hair follicles, Pacinian corpuscle, muscle spindles, and Golgi tendons.
- Efferents from first-order neurons enter the spinal cord medially via the dorsal root.
- Fibers ascend in the dorsal columns as:
- Fasciculus gracilis (medial): carries sensation from the lower extremities and terminates in the nucleus gracilis in the caudal medulla.
- Fasciculus cuneatus (lateral): carries sensation from the upper limbs and terminates in the nucleus cuneatus in the caudal medulla.
- Second-order neurons in the nuclei gracilis and cuneatus give rise to internal arcuate fibers, which cross to the contralateral side in the medulla.
- After crossing, these fibers ascend as the medial lemniscus.
- The medial lemniscus terminates in the ventral posterolateral nucleus (VPL) of the thalamus, which contains the third-order neurons.
- Axons from the VPL ascend through the posterior limb of the internal capsule and terminate in the primary somatosensory area in the postcentral gyrus.
The dorsal and ventral spinocerebellar tracts carry unconscious proprioception information from muscles and joints of the lower extremity to the cerebellum. The spino-olivary tract carries information from the Golgi tendon organs to the cerebellum.
Note: There are many important spinal cord lesions.
Blood supply of the spinal cord
The spinal cord and its associated spinal nerves are supplied by:
- A single anterior spinal artery
- Two posterior spinal arteries
The anterior spinal artery supplies the anterior two-thirds of the cord. The posterior spinal arteries supply the dorsal columns. All three spinal arteries arise from the vertebral arteries in the skull.
Segmental branches of the thoracic and abdominal aorta give off radicular branches that anastomose with the spinal arteries, providing additional blood supply. One of the largest radicular branches is the great radicular artery (artery of Adamkiewicz), which supplies the anterior spinal artery. Reduced flow through this vessel can cause spinal cord ischemia.
It’s important to avoid damaging the artery of Adamkiewicz during thoracic, abdominal, and retroperitoneal surgical procedures. Injury can lead to anterior spinal syndrome, which may present with paralysis below the level of the lesion, loss of pain and temperature at and below the level of the lesion, hypotension, erectile dysfunction, and urinary and fecal incontinence.