Cerebral blood supply
Cerebral blood supply
The brain receives blood from two main circulations:
- Anterior circulation
- Posterior circulation
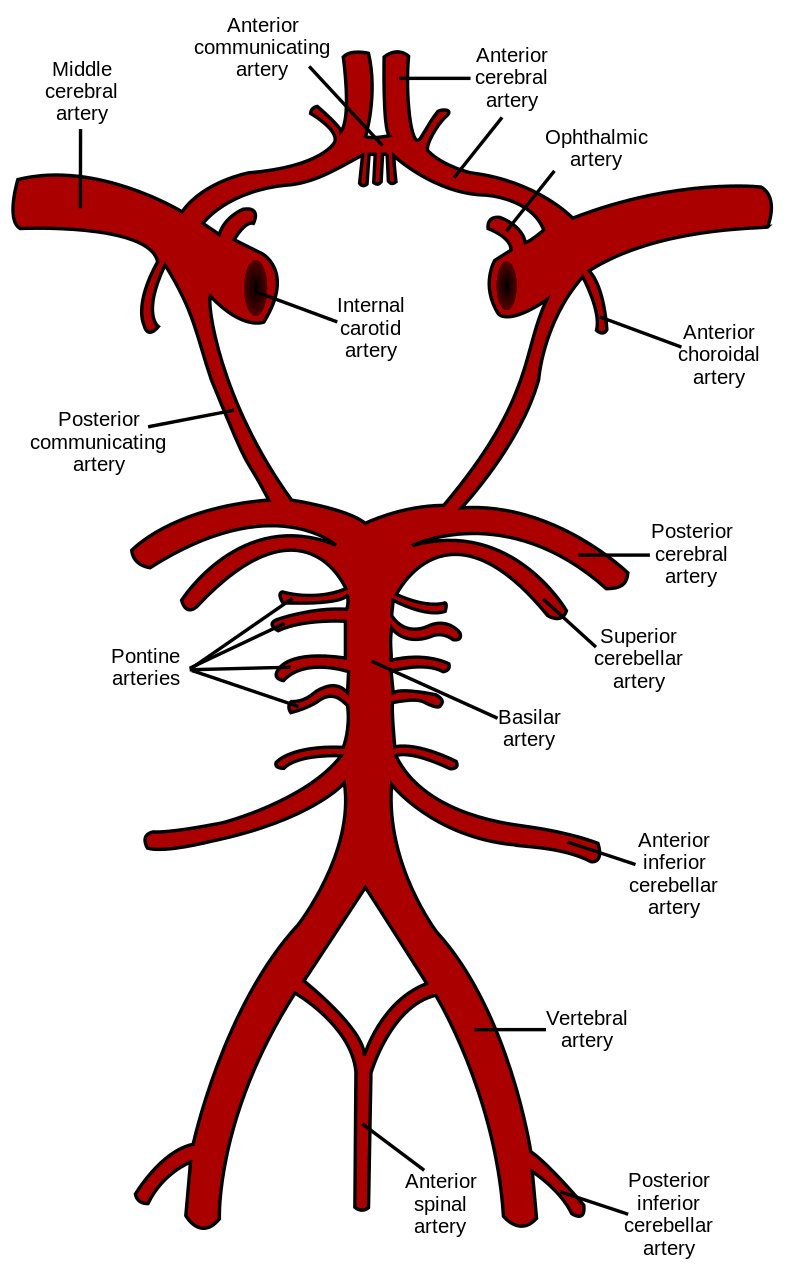
These circulations anastomose at the base of the brain to form the circle of Willis.
The internal carotid artery gives rise to the:
- anterior cerebral artery
- middle cerebral artery
- posterior communicating artery
The vertebral arteries join to form the basilar artery, which divides into:
- two posterior cerebral arteries
- superior cerebellar arteries
The following vessels form the circle of Willis:
- internal carotid arteries
- two anterior cerebral arteries connected by the anterior communicating artery
- posterior cerebral arteries
- posterior communicating arteries
- basilar artery
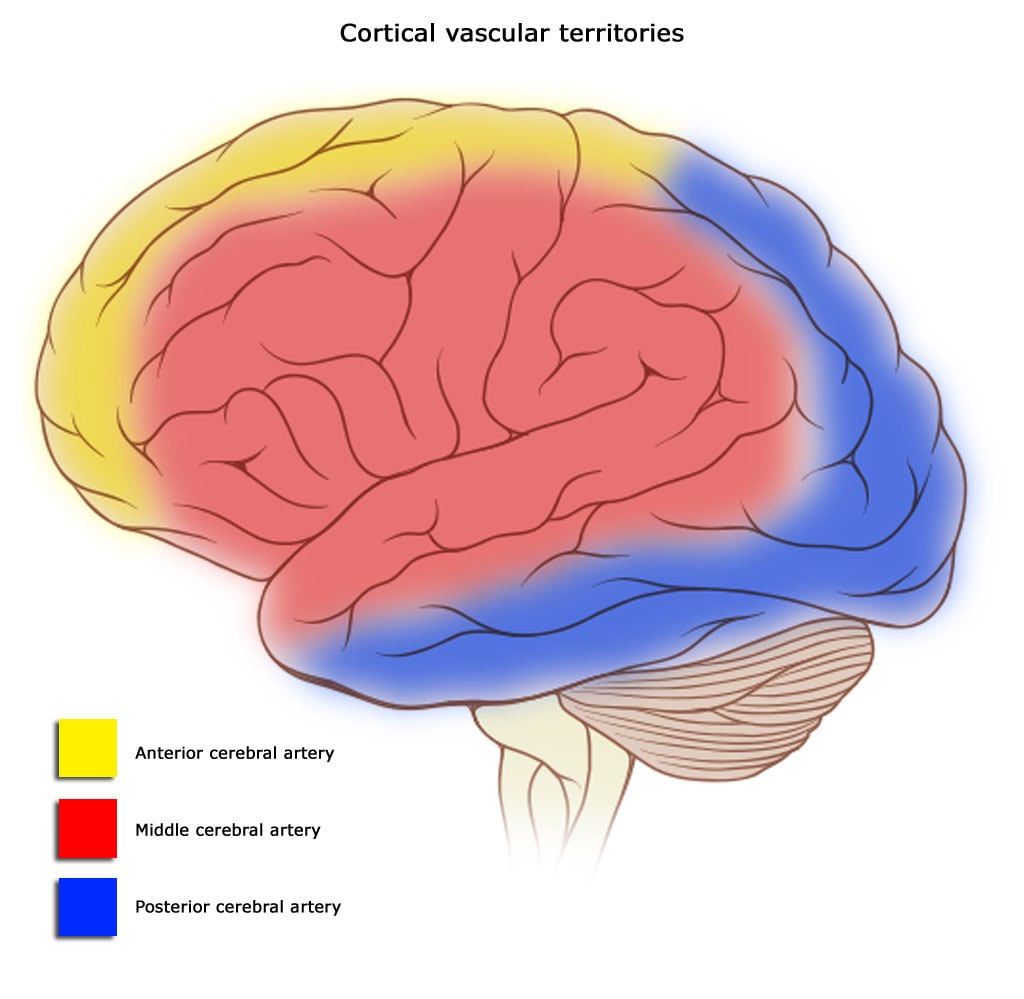
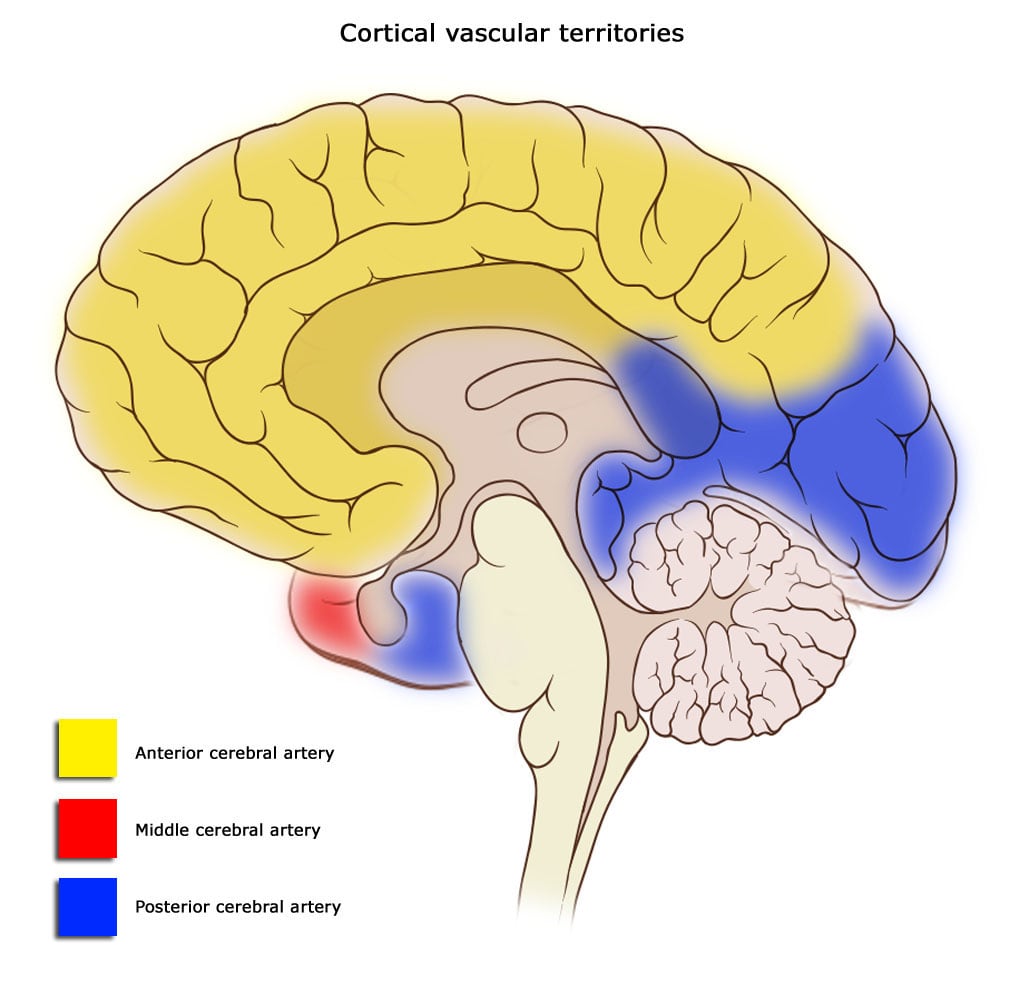
Watershed regions are areas that receive dual blood supply from the most distal branches of two large arteries. In the brain, watershed zones lie:
- between the anterior cerebral artery and middle cerebral artery
- between the posterior cerebral artery and middle cerebral artery
Because these regions are supplied by distal branches, they’re especially prone to ischemia during low-flow states (for example, after hypotension). Watershed infarcts can present as “man in barrel” syndrome, characterized by weakness that affects proximal more than distal extremities.
Cerebral venous drainage and sinuses
Cerebral veins drain into dural venous sinuses, which ultimately drain into the internal jugular veins, then into the brachiocephalic veins, and finally into the superior vena cava.
The dural venous sinuses lie between the periosteal and meningeal layers of the dura mater. Major sinuses include:
- superior sagittal sinus
- inferior sagittal sinus
- straight sinus
- transverse sinus
- S shaped sigmoid sinus
- cavernous sinus
- superior petrosal sinus
The superior sagittal sinus contains arachnoid granulations, which allow CSF to drain into venous blood. All dural venous sinuses are valveless.
Cavernous sinus
Each cavernous sinus lies lateral to the sella turcica and extends from the apex of the orbit anteriorly to the apex of the petrous temporal bone posteriorly. The body of the sphenoid bone is medial to the sinus. The sinus is divided into multiple small cave-like compartments by fibrous septa, which is why it’s called “cavernous.”
It contains several clinically important structures:
- Nerves related to the cavernous sinus: Some nerves travel in the lateral wall of the sinus. From superior to inferior, these are the oculomotor nerve (III), trochlear nerve (IV), and ophthalmic branch of the trigeminal nerve (V1). The maxillary branch of the trigeminal nerve (V2) travels either along the inferolateral aspect or just outside the cavernous sinus. The abducens nerve (VI) travels WITHIN the cavernous sinus.
- The cavernous part of the internal carotid artery runs within the sinus.
- It receives venous blood from superior and inferior ophthalmic veins, superficial middle cerebral vein and sphenoparietal sinus.
- It drains into the superior and inferior petrosal sinuses.
- Cavernous sinus syndrome: This syndrome occurs when the cavernous sinus itself, or any of the structures associated with it, is affected by disease. Common causes include metastatic tumors, meningiomas, pituitary tumors, nasopharyngeal malignancies invading the sinus, cavernous sinus thrombosis, and aneurysm of the cavernous part of the internal carotid artery. Infections in the danger area of face (bounded by the medial angle of the eyes, upper lip, and nose) can reach the cavernous sinus via the superior ophthalmic vein and indirectly via the facial veins. The facial vein anastomoses with the superior ophthalmic vein via the angular vein. Infection can also reach the cavernous sinus from the face via the inferior ophthalmic vein and the pterygoid venous plexus through an emissary vein. Cranial nerve VI (abducens) is usually the first nerve involved. This leads to ophthalmoplegia, eventually involving cranial nerves III and IV. Involvement of V1 and V2 causes sensory loss over the face, scalp, maxilla, nasal cavity, sinuses, and palate. Horner’s syndrome can result from involvement of the sympathetic plexus around the ICA. Compression of the parasympathetic nerve fibers in cranial nerve III can lead to fixed and dilated pupils. This condition is rapidly fatal if not diagnosed and treated promptly.
Blood-brain barrier (BBB)
The BBB protects the brain from external toxins and pathogens and helps tightly regulate the biochemical and physiological environment within the brain.
Anatomically, the BBB is formed by:
- CNS endothelial cells
- pericytes
- basement membrane
- astrocytes (especially their foot processes)
CNS endothelial cells are connected by continuous tight junctions. The molecules claudin, occludin, cadherin, and JAM / junctional adhesion molecules are important for maintaining these tight junctions.
Highly lipid-soluble substances can cross the BBB by diffusion (e.g., anesthetics). Ischemia, hypoxia, and inflammation can damage BBB integrity.
Structures in the circumventricular areas lack a BBB because they have discontinuous tight junctions, allowing mixing with systemic blood. These include:
- pituitary gland
- area postrema
- pineal gland
- choroid plexus
- median eminence
- paraphysis
- preoptic recess
The area postrema is also called the vomiting centre.