Respiratory system
The respiratory system is divided into a conducting zone and a respiratory zone. Only the respiratory zone participates in gas exchange.
- The conducting zone is composed of the nasal cavities, nasopharynx, oropharynx, larynx, trachea, bronchi, bronchioles, and terminal bronchioles.
- The respiratory zone is composed of respiratory bronchioles, alveolar ducts, and alveoli.
The nasal cavity
The nasal septum divides the nasal cavity into right and left halves.
The lateral nasal wall has three bony projections called the superior, middle, and inferior conchae. These form the three turbinates and border spaces called meatuses (superior, middle, and inferior).
- The posterior ethmoid and sphenoid sinuses drain into the superior meatus.
- The anterior ethmoid, maxillary, and frontal sinuses drain into the middle meatus.
- The nasolacrimal duct drains into the inferior meatus.
The nasal mucosa is ciliated, pseudostratified columnar epithelium. It produces IgA and IgE.
The nose has a rich blood supply from branches of the external and internal carotid arteries. The external nose is supplied by the facial artery, infraorbital artery, and ophthalmic artery.
Kiesselbach’s plexus (Little’s area) is on the anterior and inferior part of the nasal septum. It is the site of anastomoses between four major arteries:
- Anterior ethmoidal (branch of ophthalmic)
- Sphenopalatine (branch of maxillary)
- Greater palatine (branch of maxillary)
- Superior labial (branch of facial)
It is the major site of epistaxis (bleeding from the nose).
Posterior bleeding derives primarily from the posterior septal nasal artery (a branch of the sphenopalatine artery), which forms part of the Woodruff plexus. The Woodruff plexus is located on the lateral nasal wall, posterior to the inferior turbinate, and is mainly a venous plexus. Posterior nosebleeds are more difficult to control and can lead to aspiration.
The pharynx
The pharynx is a common passage for the alimentary and respiratory tracts. It is divided into the nasopharynx, oropharynx, and laryngopharynx.
The pharynx receives the auditory (eustachian) tube, which connects it to the middle ear. Infections can spread from the pharynx to the middle ear through this route.
The nasopharynx also contains the nasopharyngeal tonsils (adenoids) on the posterior wall. The adenoid tonsil is supplied by the ascending palatine branch of the facial artery, ascending pharyngeal artery, pharyngeal branch of the internal maxillary artery, artery of the pterygoid canal, and the ascending cervical branch of the thyrocervical trunk.
The oropharynx extends from the nasopharynx to the epiglottis. It contains a lymphatic ring of nasopharyngeal, tubal, palatine, and lingual tonsils. The palatine tonsil is supplied by the tonsillar and ascending palatine branches of the facial artery, the ascending pharyngeal artery, the dorsal lingual branch of the lingual artery, and the palatine branch of the maxillary artery.
The laryngopharynx ends at the cricoid cartilage.
The wall of the pharynx has an external circular and an internal longitudinal layer of muscles.
- The external muscles are constrictors.
- The internal muscles include the stylopharyngeus and palatopharyngeus muscles.
The larynx
The larynx extends from the C3 to C6 vertebrae.
The larynx has three single and three paired cartilages: thyroid, cricoid, epiglottic, arytenoid, corniculate, and cuneiform cartilages.
The thyroid cartilage is superficial and can be seen and palpated as the “Adam’s apple”. The cricoid cartilage is at the level of the C6 vertebra.
In cricothyrotomy, the cricothyroid membrane is incised to access the larynx in an emergency to establish patency of the airway when endotracheal intubation is not possible.
The trachea
The trachea begins at the lower edge of the cricoid cartilage and ends at the level of the T4 vertebra and sternal angle, at the carina, where it divides into the right and left main bronchi.
The trachea is located anterior to the esophagus. It is incompletely surrounded on the anterior and lateral sides by about 15-20 C-shaped hyaline cartilages. These provide flexibility and help keep the trachea open, preventing airway collapse.
The trachealis muscle (smooth muscle) runs along the posterior wall. The posterior wall is devoid of cartilage, allowing the esophagus (posterior to the trachea) to expand during swallowing.
The trachea is lined by respiratory epithelium: ciliated, pseudostratified columnar epithelium with goblet cells. The mucosal lining also contains:
- Brush cells with numerous microvilli on their surface
- Endocrine APUD cells, which regulate secretion from goblet cells and mucosal glands
- Basal cells, which are stem cells with high mitotic potential
The lobes of the thyroid gland are anterolateral to the cervical trachea, and the thyroid isthmus crosses the trachea anteriorly at the level of the second or third tracheal rings.
Bronchi, bronchioles, alveolar ducts and alveoli
There are two main bronchi.
- The right main bronchus is wider and more vertical (so there is more risk of aspiration).
- The left main bronchus is more horizontal.
The main bronchi divide into lobar bronchi.
- There are two left lobar bronchi and three right lobar bronchi.
The lobar bronchi divide into segmental bronchi, which supply the bronchopulmonary segments.
The bronchi are lined by respiratory epithelium, as described above. They have a prominent layer of circular smooth muscle. Hyaline cartilages are present in the wall.
The bronchioles are lined by simple ciliated columnar epithelium with goblet cells and Clara cells.
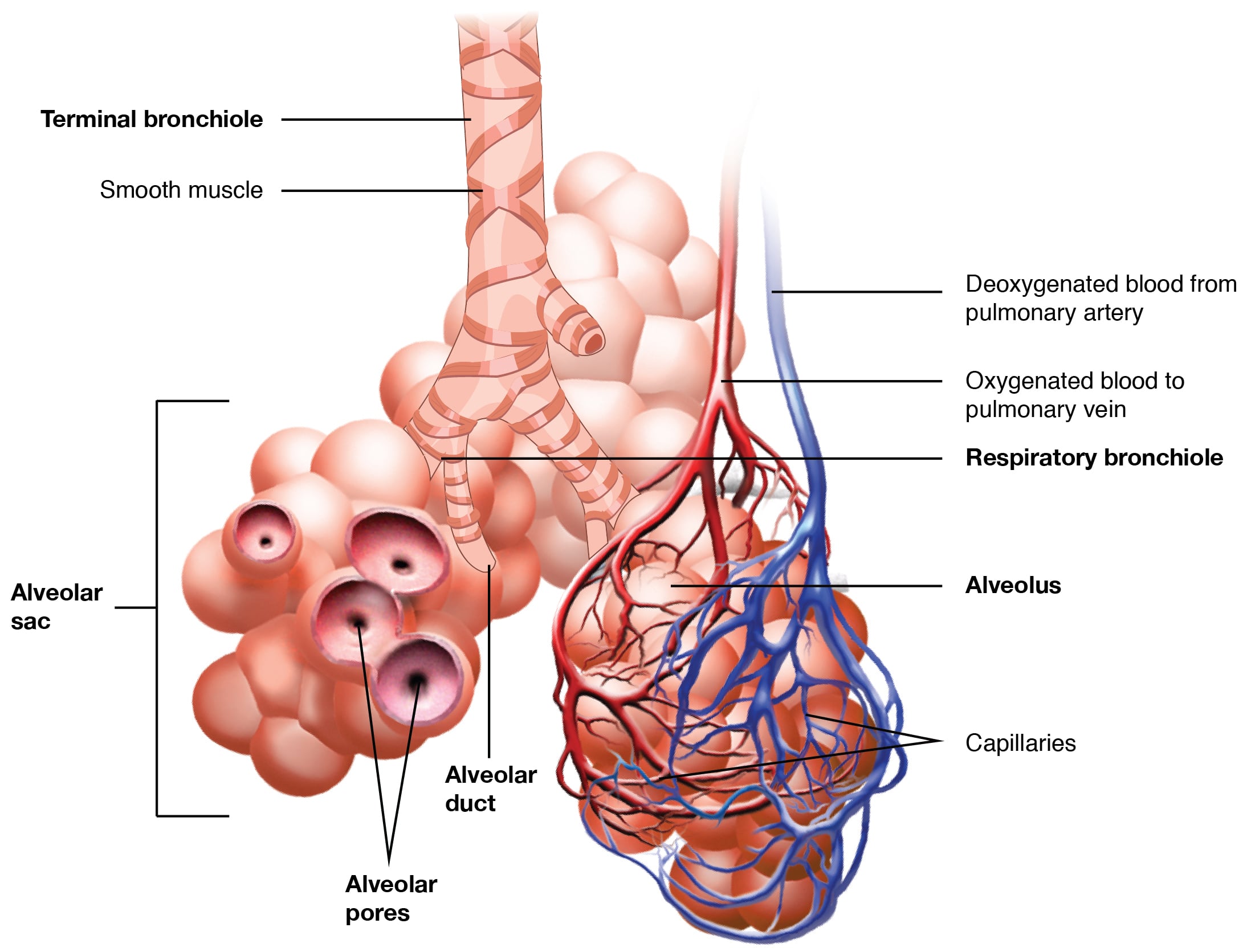
The terminal and respiratory bronchioles are lined by simple, ciliated, cuboidal epithelium with Clara cells. Cartilage is absent in the respiratory bronchioles. Occasional alveoli open into the terminal and respiratory bronchioles.
Alveolar ducts are tubular structures lined by simple squamous epithelium. The alveolar ducts are lined by alveoli. Cilia are absent in the epithelium of the alveolar ducts and alveoli.
Alveolar ducts connect to alveolar sacs, which give rise to clusters of alveoli. A network of capillaries surrounds the alveoli.
The alveolar lining is made mainly of two types of cells: type I and type II pneumocytes.
- Type I pneumocytes are flattened, simple squamous cells joined together by tight zonula occludens.
- Type II pneumocytes are cuboidal cells. They secrete surfactant, which is stored as lamellar bodies. They are also stem cells and undergo hyperplasia in response to alveolar injury and repair.
Alveolar macrophages are present in the septae.
Pores of Kohn are present in the interalveolar septum. Their role is collateral ventilation and equalization of pressure across the alveoli. They also form channels for the spread of infections like pneumonia and in cancers.
Sometimes, alveolar brush cells are called type III pneumocytes. Their role is ill defined.
Blood air barrier
The blood air barrier is formed by the surfactant layer, type I pneumocyte, basement membrane, and capillary endothelial cell. Diffusion occurs across the blood air barrier.
Lungs
Both lungs are divided into lobes by fissures: 3 on the right and 2 on the left.
The right lung is further divided into 10 segments:
- 3 in the upper lobe
- 2 in the middle lobe
- 5 in the lower lobe
The left lung has 8 segments:
- 4 in the upper lobe
- 4 in the lower lobe
Aspiration pneumonia occurs in the apical segment of the lower lobes (right more common) and the posterior segment of the upper lobes in a supine patient. In the erect position, aspiration pneumonia occurs in the basal segment of the lower lobe (right more common).
Surface anatomy
Surface anatomy is important for assessing thoracic and abdominal injuries and for procedures like thoracotomy.
The apices of the lungs extend 3 cm above the medial third of the clavicle.
The inferior margins of the lung are at:
- T6 in the midclavicular line
- T8 in the midaxillary line
- T10 posteriorly
The parietal pleura is situated about two vertebral levels lower than the lung margins.
The upper lobe of the right lung extends up to the fourth rib, the middle lobe extends from the fourth to sixth ribs, and the lower lobe is below the sixth rib. On the left, the upper lobe extends to the sixth rib, and the lower lobe is below it.
- Anteriorly, the upper and middle lobes of the right lung and the upper lobe of the left lung can be auscultated.
- Posteriorly, the lower lobes of the right and left lungs are auscultated.
Important receptors of the lung
- Pulmonary stretch receptors: They are present in the airway smooth muscle and are stimulated by inflation. They cause bronchodilation and inhibition of inspiration. They are innervated by myelinated vagal fibres.
- J receptors: They are present in the alveolar wall and are stimulated by inhalation of irritant gases, pulmonary edema, and microembolism. They are responsible for the sensation of dyspnea. They cause rapid, shallow breathing when stimulated and are innervated by unmyelinated vagal fibres.
- Irritant receptors: They are present in the epithelial layer, are innervated by myelinated vagal fibres, and are stimulated by dust, irritants, pneumothorax, bronchoconstriction, atelectasis, etc. They result in hyperventilation, tachypnea, and bronchoconstriction.
- Cough receptors: These are present in the trachea, large airways, pharynx, pleura, diaphragm, ear canal, pericardium, and stomach. They respond to chemical and physical stimuli to initiate the cough reflex. Cough is a protective response and helps in clearing of the airways.