Lower limbs
Sciatic nerve and branches
The sciatic nerve is the largest nerve in the human body. It arises from the ventral rami of spinal nerves L4-S3 (lumbosacral plexus). It travels posteriorly in the lower limb, continuing down toward the heel. Near the popliteal fossa, it divides into the tibial nerve and the common peroneal (fibular) nerve.
- The tibial nerve continues in the posterior compartment of the leg and into the foot.
- The common peroneal nerve travels into the lateral and anterior compartments of the leg and foot.
| Nerve | Muscles supplied | Actions | Sensory supply* |
|---|---|---|---|
| Sciatic Nerve** | Biceps femoris, semimembranosus, semitendinosus, ischial part of the adductor magnus (hamstrings) | Flexion of the knee and adduction of the hip | No direct sensory innervation |
| Tibial Nerve | Gastrocnemius, soleus, plantaris and popliteus, flexor hallucis longus, flexor digitorum longus, tibialis posterior | Plantar flexion and flexion of the toes | As medial and lateral plantar nerves to the sole of foot and heel |
| Common Peroneal Nerve | Tibialis anterior, extensor hallucis longus, extensor digitorum longus, peroneus longus, brevis and tertius | Dorsiflexion of the foot, toe extension and eversion of the foot | As superficial peroneal nerve to the posterolateral part of leg and dorsum of the foot. As deep peroneal nerve to skin between first and second toes |
- Lumbar plexus formed by the ventral rami of L1-4 plays the main role in sensory supply of the thigh. Lateral femoral cutaneous nerve supplies lateral thigh; femoral nerve supplies anteromedial thigh and anteromedial leg, medial ankle and medial foot via the anterior femoral cutaneous nerve and saphenous nerve respectively; distal third of medial thigh by obturator nerve.
** The posterior cutaneous nerve of thigh runs with the sciatic nerve and supplies sensory innervation to the posterior thigh and inferior buttocks. The sural nerve is formed by contributions from tibial and common peroneal nerves and is sensory to the calf and a small area along the lateral foot.
Sciatica
Sciatica is low back pain associated with radiating pain down the buttocks and posterior lower limb in the distribution of the sciatic nerve. The pain is typically shooting or burning, varies in intensity, and may be accompanied by muscle weakness and numbness.
Any condition that impinges on or irritates the sciatic nerve can cause sciatica, for example:
- Lumbar disc prolapse
- Lumbar spinal stenosis (typically bilateral sciatica)
- Spondylolisthesis
- Osteoporosis
- Pregnancy
- Piriformis syndrome
Acute Compartment syndrome
Acute compartment syndrome occurs when intracompartmental pressure increases enough to interfere with local circulation. It can occur anywhere a compartment is present (e.g., arm, forearm, hand, abdomen, lower limbs).
Common causes include:
- Local trauma
- Fractures
- Repetitive exercise
- Burns
- Gunshot wounds
- Tight splints
Clinical features include local pain out of proportion to the injury (often worse with passive stretching), numbness, possibly absent pulses, and local edema and swelling. Treatment is early decompression with fasciotomy.
Tarsal tunnel syndrome
Tarsal tunnel syndrome is caused by compression of the tibial nerve or its branches as it passes through the tarsal tunnel under the flexor retinaculum at the ankle. It presents with pain, tingling, and numbness radiating from the ankle medially into the ankle and foot.
Peroneal nerve injuries
Common peroneal nerve injury causes foot drop and sensory loss in the peroneal nerve distribution. Injury is common because the nerve lies close to the skin on the lateral part of the leg, just under the knee, as it winds around the neck of the fibula.
It can occur with:
- Knee dislocations
- Tight plaster casts
- Fracture of the fibula
Deep tendon reflexes
Deep tendon reflexes are stretch reflexes modulated by muscle spindles. Reflexes are graded from 0 to 4+:
- 0: absent reflex
- 1+: weak reflex
- 2+: brisk
- 3+: very brisk
- 4+: clonus (repeating)
| Reflex | Nerve Root |
|---|---|
| Jaw jerk | Trigeminal nerve |
| Biceps jerk | C5,6 |
| Triceps jerk | C6,7 |
| Brachioradialis | C5,6 |
| Finger jerk | C8-T1 |
| Knee jerk | L3,4 |
| Ankle jerk | S1 |
Skeletal muscle histology
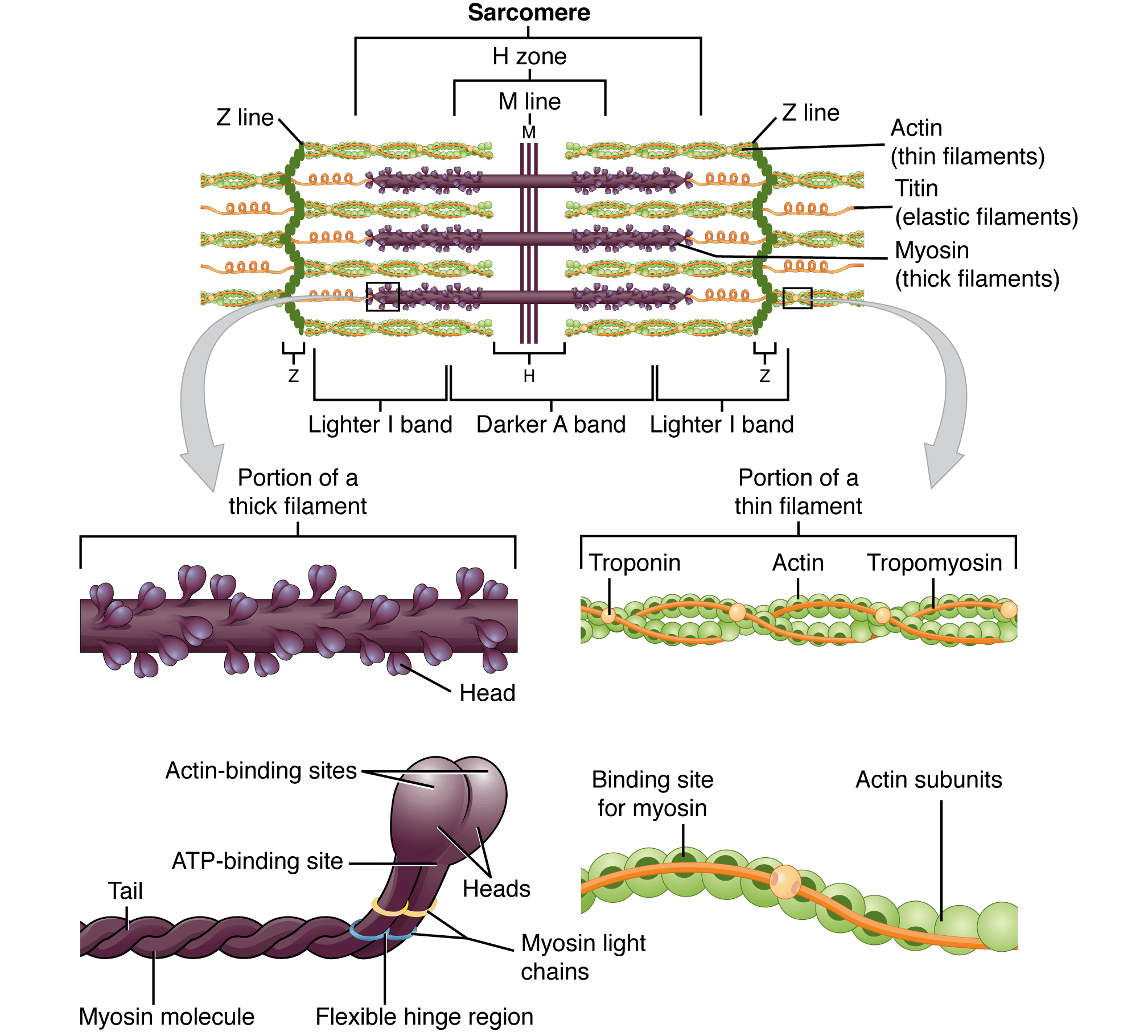
The sarcomere is the basic functional unit of muscle. Sarcomeres join end-to-end to form muscle fibers, which are covered by endomysium. Muscle fibers bundle together to form fascicles, which are covered by perimysium. Fascicles are then covered by epimysium.
Each sarcomere is bounded by Z discs. Thin actin filaments attach to the Z discs.
- The region on either side of the Z disc contains thin filaments only and is called the I band (light band).
- Between two I bands is the A band.
- The A band contains dark regions formed by overlapping thin and thick (myosin) filaments, and it includes the M line and H zone.
- The M line is in the center of the sarcomere and anchors the thick filaments.
- The H zone contains only thick filaments.
During muscle contraction:
- The sarcomere shortens.
- The I band and H zone become smaller.
- The width of the A band remains the same.
- The dark band increases in size because overlap between thin and thick filaments increases.
According to the sliding filament theory of muscle contraction, myosin binds to actin and functions as a motor that drives filament sliding. This process requires energy in the form of ATP.