Miscellaneous disorders
-
Multiple myeloma (MM): MM is a malignant, monoclonal proliferation of plasma cells in the bone marrow. It’s more common in older Black men. Exposure to X-rays and other ionizing radiation increases the risk. Translocations involving chromosome 14 are associated with MM.
In MM, malignant plasma cells proliferate and produce an excess of M protein (most often IgG or IgA; less commonly IgD or IgE). Plasma cells also produce excess kappa or lambda light chains, called Bence Jones proteins. Bence Jones proteins precipitate when heated to 40-60°C and re-dissolve at 100°C.
Because normal immunoglobulins aren’t produced in sufficient amounts, immunodeficiency occurs.
Osteolytic bone lesions develop due to increased osteoclast activity and decreased osteoblast activity. Clinical symptoms include fatigue, fever, bone pain (especially in the back and ribs), frequent infections, easy bleeding, fractures, paresthesias, and dyspnea.
Renal disease can occur from deposition of Bence Jones proteins in the distal convoluted tubule. AL amyloidosis and hyperviscosity syndrome may occur. Increased serum beta-2 microglobulin is associated with a poor prognosis.
CRAB symptoms for the diagnosis of multiple myeloma
- C for Calcium elevation or hypercalcemia
- R for Renal insufficiency
- A for Anemia
- B for Bone disease
Bone marrow biopsy reveals >10% myeloma cells. Myeloma cells may appear:
- Mature, with an eccentric “cartwheel” nucleus, or
- Immature, with a prominent nucleus and nucleoli
Dutcher bodies (intranuclear inclusions) and Russell bodies may be present. Myeloma cells are CD138+ and CD56+.
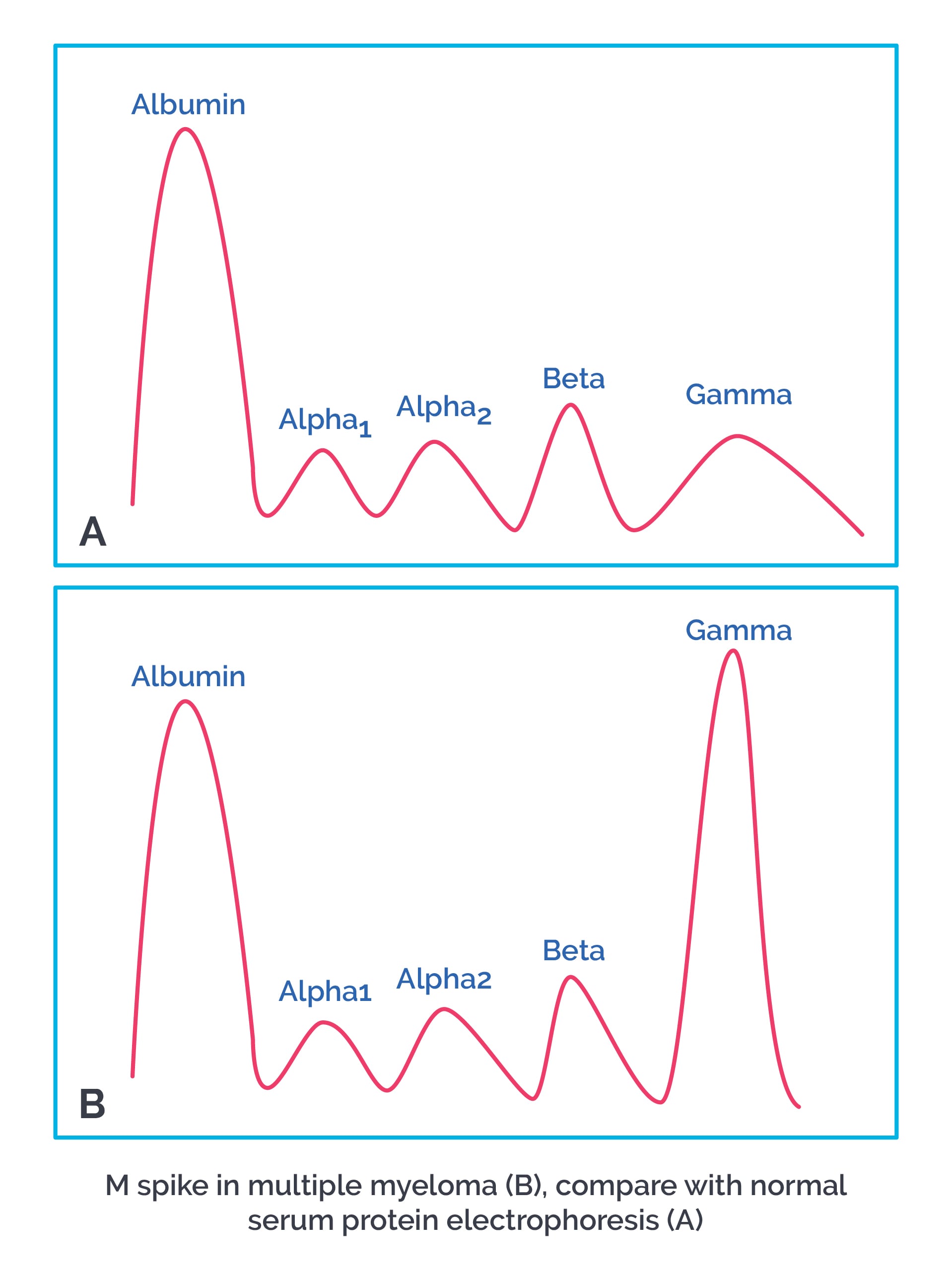
Urine shows Bence Jones proteins (either kappa or lambda light chains). Serum protein electrophoresis shows an abnormal M spike from M protein. ESR is high and correlates directly with prognosis.
{`A bone marrow biopsy showing >10% myeloma cells can also be seen in **smoldering MM (SMM)**, an intermediate clinical stage between MGUS and MM. SMM lacks the CRAB symptoms seen in MM, although Bence Jones proteins are present.
MM can rarely progress to **plasma cell leukemia**. In this case, **>20% of blood cells** are myeloma plasma cells, and there is involvement of other organs.
Treatment of MM is with combination chemotherapy such as melphalan, bortezomib, daratumumab, prednisone, doxorubicin, lenalidomide, interferon therapy, and bone marrow transplantation.
`}-
Monoclonal gammopathy of unknown significance (MGUS): MGUS is a premalignant condition seen in older age groups. It is characterized by:
- Elevated serum M protein
- <10% plasma cells in the bone marrow
- Absence of CRAB symptoms
An M spike is seen on electrophoresis. Patients may report fatigue, weakness, or dementia-like changes. MGUS progresses to MM at a rate of 1-2% of patients per year, so follow-up is needed to detect progression.
-
Waldenstrom macroglobulinemia: This is a monoclonal, malignant proliferation of B lymphocytes that secrete heavy IgM macroglobulins. It presents with peripheral neuropathy, lymphadenopathy, hepatosplenomegaly, and hyperviscosity syndrome (with visual deficits), along with weakness, fatigue, anemia, and bleeding tendencies.
Bone marrow biopsy shows infiltration with cells of varied morphology, including lymphocytes, plasma cells, mast cells, and histiocytes. Electrophoresis shows an M spike from IgM. ESR is high.