Macrocytic anemias
Macrocytosis refers to a condition in which RBCs are larger than normal, with an MCV >100 fL. Macrocytes can be seen on a peripheral blood smear. Macrocytosis may be physiological in newborns, infants, and pregnant women. When macrocytosis and anemia coexist in the same person, the condition is called macrocytic anemia. Macrocytic anemia may be megaloblastic or non-megaloblastic.
Megaloblastic anemia is seen in Vit B12 or folate deficiency, pernicious anemia, and transcobalamin II deficiency. It causes defects in DNA synthesis, cellular proliferation, and maturation, with relatively little effect on RNA and cytoplasm synthesis. Vit B12 and folate deficiency can be seen with dietary deficiency. B12 deficiency is more common in vegetarians and can also occur following gastrectomy, blind loop syndrome, and pernicious anemia. Rarely, Diphyllobothrium latum infestation can cause B12 deficiency. When vitamin B12 is deficient, folic acid can’t be converted to its active form. Vit B12 deficiency typically takes a few years to manifest, while folate deficiency typically takes only a few months.
Megaloblastic anemia due to vitamin B12 deficiency presents with fatigue, headache, palpitations, and dyspnea, along with neurological symptoms such as dysesthesia and hypoesthesia. Other findings include glossitis and gray hair. In severe cases, subacute combined degeneration may occur, with ataxia and decreased proprioception and vibration sensation. Neurologic symptoms are typically absent in folate deficiency anemia.
In megaloblastic anemia, large, oval RBC precursors called megaloblasts with an immature, “lacy” nucleus can be seen in the bone marrow. The bone marrow is hypercellular. The peripheral smear shows hypersegmented neutrophils (>5 lobes), macro-ovalocytes (large RBCs), poikilocytosis, and anisocytosis. Macrocytosis is the earliest abnormality seen on complete blood counts in patients with folate or vitamin B12 deficiency. On peripheral smear, macrocytes will be larger than the nucleus of a small lymphocyte. Reticulocyte count will be low (<2%). MCV, MCH, and RDW are increased, while MCHC is normal or decreased. Serum LDH and unconjugated bilirubin may rise.
Serum homocysteine will be elevated in folate and Vit B12 deficiencies, but methylmalonic acid will be elevated in Vit B12 deficiency only.
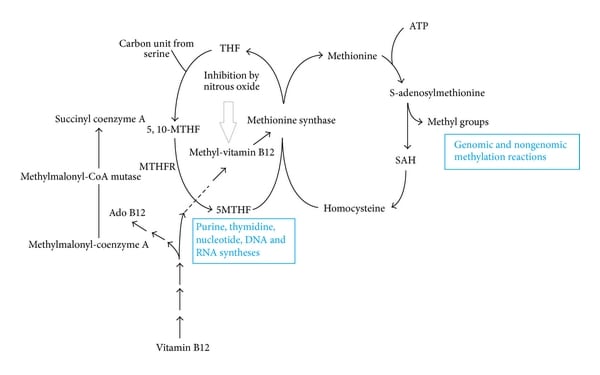
Pathways of intracellular vitamin B12 metabolism. MTHFR: methylenetetrahydrofolate reductase; 5,10-MTHF: 5,10-methylenetetrahydrofolate; 5-MTHF: 5-methylenetetrahydrofolate; THF: tetrahydrofolate; SAH: S-adenosyl homocysteine.
HoloTC II (holotranscobalamin II) is an emerging marker that may be useful in establishing a diagnosis of early vitamin B12 deficiency. RBC and serum folate levels will be low in folate deficiency. RBC folate levels are more specific for testing folate deficiency. Urinary levels of FIGLU (formiminoglutamic acid) increase after histidine administration in folate deficiency. If both Vit B12 and folate levels are normal, other causes of megaloblastic anemia should be considered.
Pernicious anemia (atrophic gastritis): Pernicious anemia is an autoimmune gastritis characterized by anti-parietal cell and anti-intrinsic factor antibodies. Antibodies to H+/K+ATPase are seen. It mainly affects the gastric body and fundus. It manifests with hypochlorhydria (decreased gastric acid) production and Vit B12 deficiency anemia. Hypochlorhydria induces feedback hypergastrinemia. It may be associated with other autoimmune diseases such as type 1 diabetes, autoimmune thyroiditis, and Addison’s disease. Patients with pernicious anemia are at high risk of developing gastric adenocarcinoma and carcinoid tumors. Treatment is lifelong parenteral Vit B12 administration.