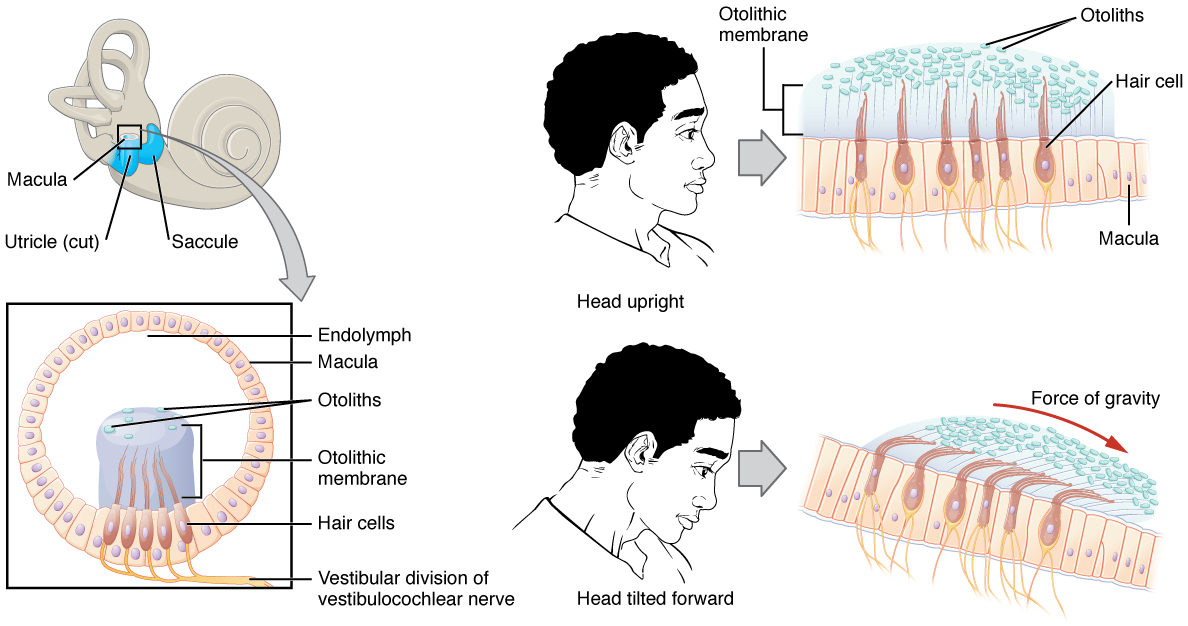

Vestibular system
Vestibular disorders
Generalized symptoms of vestibular disorders are as follows:
- Dizziness
- Balance deficits
- Vertigo
- Blurred vision
- Recurrent falls
- Nausea and vomiting
The examination for vestibular dysfunction is critical in determining the type and the treatment options.
The following are ways to determine the type of disorder:
- Inquire about symptoms and duration of symptoms
- Conduct vestibular ocular- reflex testing by assessing nystagmus, clarity of vision with head movements , and body movements
- Vertebral artery testing
- Sensory testing
- Clinical test of sensory interaction on balance (CTSIB)
- Functional testing- transfers, gait, dynamic sitting, and dynamic balance
- Vestibulospinal reflex testing: examining the posture and balance in all positions
- Positional changes and their impact on symptoms
- Cervical range of motion
- Outcome measures as appropriate, such as the dynamic gait index
Central vestibular disorders
Central vestibular dysfunction symptoms include:
- Nystagmus in vertical, horizontal, or rotational planes
- Non-fatigable nystagmus
- No hearing loss or tinnitus
- Vertigo is sometimes present
- Disequilibrium is severe
- Can be associated with other cranial nerve or cerebellum signs
- Visual fixation and head position have no impact
Treatment for central vestibular dysfunction:
- Identify triggers, if any, that are noted to be external
- Gaze stabilization exercises to assist with improving the vestibular ocular reflex
- Coordination activities to address cerebellar symptoms
- Adaptation exercises to decrease dizziness to allow for retraining of the brain
- Substitution of visual and somatosensory systems in the presence of vestibular dysfunction
Peripheral vestibular dysfunction
Symptoms of peripheral vestibular dysfunction
- Nystagmus is horizontal and torsional
- Nystagmus decreases with visual fixation
- Nystagmus is fatiguable and lasts less than one minute
- Vertigo is always present
- Loss of hearing
- Ringing in the ears
- Disequilibrium
- Feeling of fullness in the ear
Differential diagnosis of peripheral vestibular dysfunction with intervention strategies
Benign paroxysmal positional vertigo (BPPV)
- Benign paroxysmal positional vertigo (BPPV)
- An endolymph disorder causing brief, intense vertigo due to head position change- the otoconia within the semicircular canals become dislodged
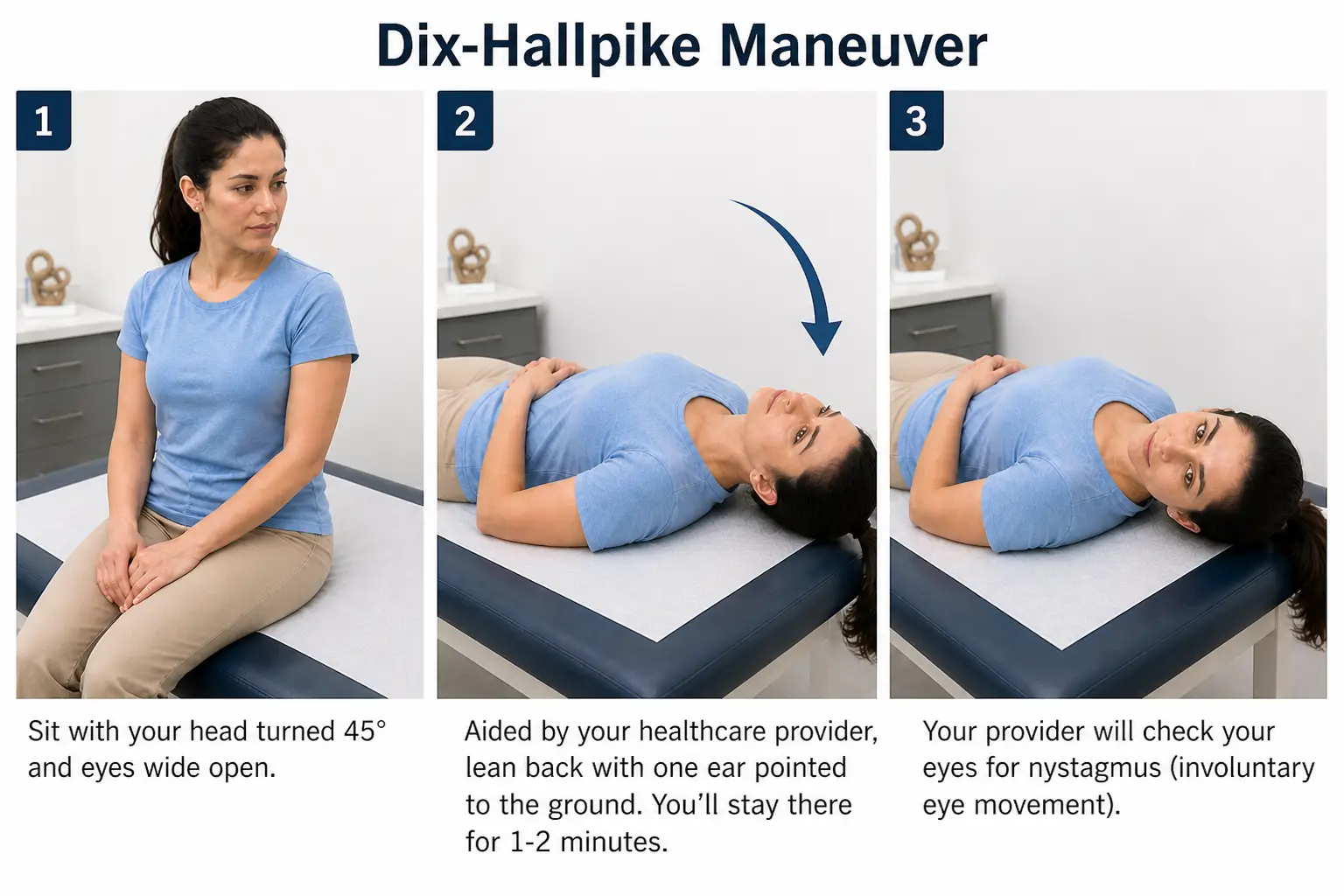
- Confirmation of BPPV is done by performing the Dix-Hallpike - before completing, the therapist must perform a vertebral artery test and ensure appropriate cervical range of motion is present
- Patient positioned in a long sitting with head turned to 45 degrees towards the affected side
- Patient is quickly lowered to supine with head remaining in 45 degrees and hanging over the edge of the mat- therapist is observing for nystagmus
- Nystagmus will resolve within 30-60 seconds
- A positive test occurs when the patient experiences nystagmus and vertigo with a head position change
- Repeat test on contralateral side
Understanding what nystagmus means in relation to BPPV
- Ageotrophic
- Fasting beating phase of the nystagmus is moving away from the ground (towards the upper ear)- this indicates lateral canal BPPV
- Geotropic
- Fast beating phase of nystagmus is moving towards the ground (towards the lower ear) - this indicates posterior canal BPPV
Differentiation of BPPV and canals impacted
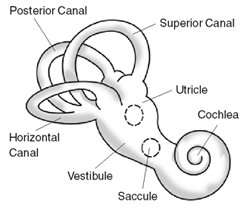
- Lateral canal BPPV
- Can manifest as ageotrophic or geotrophic horizontal nystagmus
- Treatment is with the ith log roll maneuver or barbeque roll to move otoconia into position (treatments are performed as home exercise programs)
- Log roll maneuver
- Lie on your back with your head centered and neck flexed about 30 degrees
- Turn your head 90 degrees toward the affected ear
- Hold for 30 seconds, or until vertigo and nystagmus stop
- Turn your head back to center
- Turn your head 90 degrees away from the affected ear
- Lie on your stomach with your elbows bent
- Roll back onto your back toward the affected ear
- Barbeque roll maneuver (only for left lateral canal BPPV)
- Lie on your left-hand side and wait for 30 seconds.
- Roll onto your back and wait for 30 seconds.
- Roll onto your right-hand side and wait for 30 seconds.
- Tuck your chin down slightly. Roll onto your stomach and prop yourself up on your elbows. Wait for 30 seconds.
- Roll onto your left-hand side and wait for 30 seconds.
- Slowly return to a sitting position. Keep your chin level.
- Sit for five minutes, and then repeat the previous step
- Sit for 15 minutes to finish.
- Posterior canal BPPV (most common BPPV)
- Typically presents with rotary, geotrophic nystagmus
- The epley maneuver is performed to reposition the otoconia
- Sit in a long sitting position
- Turn your head toward the side that causes vertigo.
- Quickly lie you down on your back with your head in the same position just off the edge of the table. You will likely feel more intense vertigo symptoms at this point.
- Slowly move your head to the opposite side.
- Turn your body so that it is in line with your head. You will be lying on your side with your head and body facing to the side.
- Sit upright.
- Anterior canal BPPV (least common BPPV)
- Typically presents with vertical downbeat nystagmus
- The Yacovino maneuver is performed to reposition otoconia
- Sit on the edge of a bed with your head in a neutral position.
- Quickly lie back onto your back, allowing your head to hang slightly below horizontal, ensuring your neck is supported by the bed.
- Stay in this head-hanging position until dizziness subsides, usually for 30 seconds or more.
- While still lying down, slowly move your head into a chin-to-chest position, keeping your body relaxed.
- Slowly return to a sitting position while maintaining the chin-to-chest position
- Log roll maneuver
Meniere’s disease
The management of symptoms includes
- Low sodium diet- to reduce fluid levels
- Regular exercise- improve balance and reduce stress
- Management of stress- can exacerbate an episode of vertigo
- Diuretics- reduce the fluid within the ear
- Surgery- drain excess fluid or remove the damaged portion of the inner ear
Physical therapy management of individuals with Meniere’s disease is symptom-based, and episodes of care are short. The focus will primarily be to assist with any balance deficits, muscle weakness, provide an individualized home exercise program, and reinforce patient education.
Vestibular neuritis
Treatment options will include:
- Antibiotics for the management of infection
- Corticosteroid medication for the management of inflammation
- Anti-nausea medication for persistent nausea and vomiting
Physical therapy interventions to treat vestibular neuritis are rare, as the symptoms resolve quickly. If any balance or coordination deficits continue, then physical therapy interventions will be prescribed at that time.
Labyrinthitis
Treatment interventions include:
- Antihistamines reduce the vertigo symptoms
- Anti-nausea drugs for treatment of nausea and vomiting
- Corticosteroids for treatment of inflammation
- Antibiotics for treatment of infection