
Interventions for neurological conditions
Principles of motor learning/motor control
Strategies for motor learning
Motor learning strategies are required when attempting to learn a new skill through a combination of mass practice and experience. Specific strategies for how to assist an individual with learning a new skill are as follows:
- Practice skill
- Begin skill practice with guided imagery — kinesthetic learning (passive movement)
- Initially blocked schedule practice progressing to variable schedule practice, to finally progressing to random schedule practice as practice repetitions increase and learning improves
- Provide effective feedback
- Begin with extrinsic feedback
- Progress to intrinsic feedback with augmented feedback
- The types of augmented feedback are knowledge of results and knowledge of performance
- Types of feedback schedules
- Feedback given after completion of every task (early stage of learning)
- Summed feedback— feedback given after a set number of attempts
- Fading feedback— decreasing the amount of feedback given to none as appropriate
- Bandwidth feedback- feedback only given if movement is outside of the designated range
- Transfer specific skill to be generalized in various environments
- Skill acquisition leads to the skill being applied in varied situations and environments successfully
- This occurs after the patient is deemed proficient in the original skill
Stages for motor learning
Stages by which motor skill acquisition follows.
- Cognitive — ”What to do” stage
- Learner develops understanding of tasks and how to perform
- Movements are slow and inconsistent; there exists an increased amount of trial and error
- Extrinsic feedback only
- Blocked scheduling
- Consistent feedback after each trial of movement
- Associative — “How to do” stage
Learner practices and refines movement
- Learner begins to understand errors of movement
- 50% extrinsic feedback and 50% intrinsic feedback
- Continue with blocked scheduling and progressing to variable as skill acquisition occurs
- Feedback should progress from summed to faded or decreasing over time.
- Learner begins to understand errors of movement
- Autonomous — “How to succeed” stage
- Skills performed automatically and with minimal conscious error
- Highly skilled and consistent performance
- Intrinsic feedback only
- Random practice schedule
- If any feedback, bandwidth feedback given
Task-specific training
Examples of task-specific training
- Locomotor training
- Motorized treadmill training with partial body weight support to promote early gait training
- This activity is used to assist with meeting the needs of the patient based on their current functional status to return to baseline
- Constraint-induced movement therapy (CIMT)
- Utilized post-stroke to constrain the unaffected upper extremity by use of a protective hand mitt
- The goal is to constrain the unaffected extremity and force the use of the affected limb to be utilized
- Utilized post-stroke to constrain the unaffected upper extremity by use of a protective hand mitt
Proprioceptive neuromuscular facilitation (PNF)
Rhythmic initiation
- A progression of movement from passive → active-assisted → active → resisted. This technique is used to improve the initiation and coordination of movement.
- Example:
- Patient: A person with Parkinson’s disease.
- Application: The Therapist helps initiate movement for rolling from supine to side-lying, gradually allowing the patient to take over the movement and eventually providing resistance for strengthening.
Rhythmic rotation
- Slow, passive rotational movements around a longitudinal axis are applied to reduce hypertonia (increased muscle tone) and promote relaxation.
- Example:
- Patient: An individual with spasticity in the trunk.
- Application: The Therapist slowly rotates the patient’s trunk to assist in relaxing the muscles before initiating trunk flexion activities.
Rhythmic stabilization
- This involves isometric contractions of antagonist muscle groups simultaneously to improve joint stability and postural control.
- Example:
- Patient: A patient sitting unsupported.
- Application: The Therapist applies multidirectional resistance to the patient’s shoulders, challenging them to maintain their posture and improve trunk stability.
Approximation
- Gentle compression of joint surfaces, typically in weight-bearing positions, to stimulate mechanoreceptors and enhance postural stability and muscle activation around the joint.
- Example:
- Patient: A person in a quadruped position or standing.
- Application: The Therapist gently compresses the patient’s shoulder joints during weight-bearing to promote co-contraction and stabilize the joint.
Slow reversals
- Alternating concentric contractions of agonist and antagonist muscles without relaxation to improve coordination and ensure smooth transitions between movements.
- Example:
- Patient: A patient with knee weakness.
- Application: Therapist resists knee flexion, then extension in a seated position, alternating back and forth to improve functional control and coordination.
Hold-relax
- An isometric contraction of a muscle group followed by relaxation and passive stretching. This technique is particularly useful for improving the range of motion when pain or tightness is present.
- Example:
- Patient: A person with hamstring tightness.
- Application: The patient performs an isometric contraction of the hamstrings against resistance, followed by passive stretching to improve flexibility.
Contract-relax
- An isotonic contraction of the muscle through its available range, followed by relaxation and passive movement into an increased range of motion to improve flexibility.
- Example:
- Patient: A person with limited hip range of motion.
- Application: The patient resists the therapist’s push into hip extension and then relaxes, allowing the therapist to stretch the hamstrings and improve flexibility.
Repeated contractions
- This involves repeated quick stretches followed by resisted contractions to enhance the initiation and strength of weak muscles.
- Example:
- Patient: A person with weakness in shoulder flexion.
- Application: The therapist provides a quick stretch to the anterior deltoid, followed by resistance to strengthen the muscle and improve the range of motion.
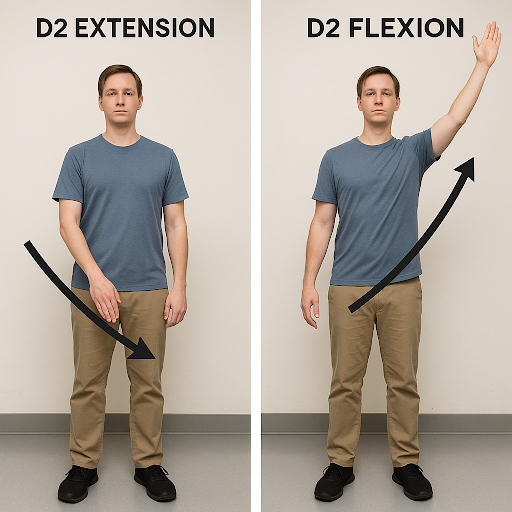
PNF patterns are associated with the way in which the joints are moved to perform specific patterns outside of synergy. PNF patterns exist for both the upper and lower extremities. The patterns are as follows for the upper extremity:
D1 flexion
D2 flexion
D1 extension
D2 extension
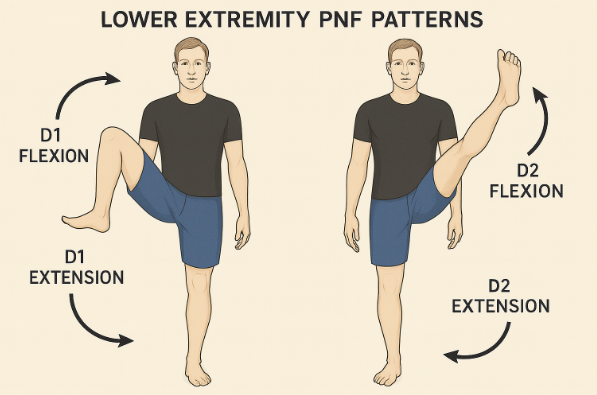
The patterns are as follows for the lower extremity:
D1 flexion
D2 flexion
D1 extension
D2 extension
Neurodevelopmental treatment (NDT)
- Developmental stages
- Each individual with neurological deficits has varied functional deficits.
The developmental stage aims to assess what is their current functional status and then aid in getting to the next stage.- Example: A stroke patient can sit independently, the next stage would be to work on standing before gait
- Each individual with neurological deficits has varied functional deficits.
- Sensory integration
- Providing individuals with neurological deficits requires sensory input to assist with understanding of their environment and how to respond to it
- Postural control
- Emphasizing the need for appropriate postural alignment and stability to aid in improving movement patterns
- Hands-on approach
- Therapists provide tactile feedback to the given individual’s knowledge of correct movement patterns
Frenkel exercises
Description:
- Frenkel exercises are slow, repetitive, and precise movements performed in supine, sitting, and standing positions.
- They emphasize visual control to compensate for loss of proprioception.
- Movements are performed actively, and the patient is instructed to watch their limbs while moving.
- Exercises are progressed from simple to complex, and from unilateral to bilateral movements.
- Rhythm, speed, and range are gradually increased as control improves.
- Can be done with or without verbal cues and metronome guidance to aid timing.
Role in neurological rehabilitation:
- Improves coordination in patients with sensory ataxia, where proprioceptive feedback is diminished.
- Promotes motor control and timing through visual compensation and repetition.
- Enhances concentration and motor planning through attention to precise limb movement.
Example exercises:
Treatment strategies for individuals with pusher syndrome
Treatment strategies can include the following:
- Do not push/pull to correct posture
- Utilize visual cues in the environment to assist with achieving an upright position, such as door frames or windows
- This gives the individual with pusher syndrome a cue as to what is vertical
- Stand/sit with non-paretic side against the wall to provide support for vertical alignment
- Increase the weightbearing to paretic side through manual pressure techniques
- Place tape on the floor to assist with giving a visualization of vertical
- Distract the non-paretic side to avoid pushing by this extremity
Outcome measures
- Berg balance scale
- Purpose: predict the risk of falls and the prescription of an assistive device
- Setting: inpatient rehab, outpatient
- Special considerations:
- assesses the individual in static and dynamic positions in both sitting and standing
- A score of 45 or less indicates an increased fall risk
- Functional gait assessment (FGA)
- Purpose: evaluate balance and postural stability during gait
- Setting: inpatient rehab, outpatient
- Special considerations:
- Deviation of the Dynamic Gait Index (DGI) to allow for improved reliability and decrease the ceiling effect (can be used in a diversity of populations)
- A score of 22 or less indicates an increased risk for falls
- Can be used to show a change in the disease process, with a change of 4 or greater indicating a significant change in the disease process
- Dynamic gait index (DGI)
- Purpose: measures an individual’s ability to respond to changing demands beyond steady-state walking- specifically for individuals with balance and vestibular deficits
- Setting: inpatient rehab, outpatient
- Special considerations:
- Tests incorporate head turns, stepping over objects, and avoiding obstacles as testing components- may be good for high-level patients with balance deficits *A score of 19 or less is predictive of falls
- Tinetti (POMA)
- Purpose: measures balance and gait to determine an individual’s risk for falling
- Setting: inpatient rehabilitation, outpatient
- Special considerations:
- Tests static balance in chair and standing, gait, perception of balance during activities, and fear of falling
- Score of 19-23 indicates moderate fall risk, 18 or less indicates high fall risk
- Functional reach
- Purpose: measure an individual’s balance and stability as related to risk for falling
- Setting: acute care, inpatient rehabilitation, outpatient
- Special considerations:
- Reaching 10 inches or greater indicates low fall risk
- Used for individuals who demonstrate difficulty with stepping strategies and reaching outside the base of support
- Fugl-Meyer
- Purpose: evaluate and quantify motor function recovery in areas of severity of motor impairments, balance, and sensory status post stroke
- Setting: inpatient rehabilitation
- Special considerations:
- Max score is 226 points
- Goal is to demonstrate progress with intensive therapy
- There is no normal score - the goal is to increase the independence level as therapy interventions are performed
- Typically taken at initial evaluation and discharge
- Activities-specific balance confidence scale (ABC scale)
- Purpose: measure self-reported confidence level in performing without losing balance or feeling unsteady
- Setting: outpatient
- Special considerations:
- This is a self-report survey
- Confidence levels are rated by percentages
*A score of 80% or higher is high-functioning
- 50-80% is moderate functioning
- 50% or less is low functioning
- 5-time sit-to-stand
- Purpose: assesses lower limb muscle strength, balance, and functional mobility
- Setting: acute care, inpatient rehabilitation
- Special considerations:
- Norms are established by age
- 11.4 seconds for 60-69 years
- 12.6 seconds for 70-79 years
- 14.8 seconds for 80-89 years
- Norms are established by age
- Timed up and go (TUG)
- Purpose: assess mobility, balance, and walking while estimating fall risk
- Setting: inpatient rehabilitation, outpatient
- Special considerations:
- A ScA score of 10 seconds or less is considered normal
- Functional Independence Measure (FIM)
- Purpose: evaluates an individual’s level of disability and the amount of assistance needed to perform mobility and ADLs
- Setting: inpatient rehabilitation
- Special considerations:
- Consists of 18 items that aid in the development of goals for patients and give objectivity to the level of function
- There is no normal score - the goal is to increase the independence level as therapy interventions are performed
Common neuromuscular medications
- Levodopa
- Mechanism of Action: replaces dopamine in the basal ganglia- use for Parkinson’s disease
- System Interactions:
- Neurological: confusion, hallucinations, delusions, psychosis, agitation
- Baclofen
- Mechanism of Action: decreases spasticity
- System Interactions:
- Musculoskeletal: muscle stiffness, abnormal posturing, bone/joint stiffness, pain, muscle weakness
- Donepezil
- Mechanism of Action: used in the treatment of Alzheimer’s disease to slow the progression of memory loss and confusion
- System Interactions:
- Musculoskeletal: muscle cramps, weakness, tremors
- Gastrointestinal: nausea, vomiting, diarrhea, weight loss
- Neuro: Headache, seizures, dizziness
- tPA (tissue plasminogen activator)
- Mechanism of Action: dissolves blood clots, specifically for the treatment of ischemic stroke
- System Interactions:
- Gastrointestinal: Nausea, vomiting
- Neuro: Headache, dizziness, blurred vision
- Pulmonary: Cough
- Keppra
- Mechanism of Action: used to treat seizures
- System Interactions:
- Cardiac: Chest pain
- Gastrointestinal: Bloating, constipation
- Integumentary: acne
- Neuro: mood swings, dizziness, headache