Compare and contrast central nervous systems pathologies part 2
Spinal cord injury
Partial or complete disruption of the spinal cord resulting in paralysis, sensory loss, altered spinal reflexes, and altered autonomic function.
The causes of spinal cord injury can be falls, motor vehicle accidents, penetrating wounds, disc prolapse, or vascular compromise.
Pathophysiology:
- Primary injury: direct injury to the spinal cord or disruption of vascular supply
- Secondary injury: edema, demyelination, or necrosis of axons
Severity of injury:
- Complete: no sensory or motor below the level of injury; no sacral sparing
- Incomplete: inconsistent sensory or motor below the level of injury; sacral sparing present
American spinal cord injury (ASIA) levels of injury
- A- Complete
- No motor or sensory function preserved below the level of injury
- No motor or sensory in sacral segment S4-S5 (sacral sparing)
- B- Incomplete
- Sensory but no motor below the level of injury
- Sensory to sacral segments S4-S5 , but no motor to these segments
- C- Incomplete
- Motor function is present below the level of injury, with major muscles having a manual muscle test grade less than 3
- D- Incomplete
- Motor function is present below the level of injury , with major muscles having a manual muscle grade greater than 3
- E- Normal
- Motor and sensory are normal
Classifications of incomplete spinal cord injuries
- Central cord syndrome
- Etiology; Cervical hyperextension
- Deficits:
- Loss of bilateral pain and temperature sensation (spinothalamic tract)
- Loss of bilateral motor function - primarily upper extremities (corticospinal tract)
- Intact:
- Preservation of proprioception, vibratory sense, and kinesthesia (dorsal column lateral meniscus)
- Anterior cord syndrome
- Etiology C: cervical flexion, vascular compromise
- Deficits:
- Loss of motor function bilaterally below the level of injury (corticospinal tract)
- Loss of bilateral pain and temperature (spinothalamic) *Intact: preservation of proprioception, vibratory sense, and kinesthesia (dorsal column lateral meniscus)
- Brown-sequard syndrome
- Etiology: Penetrating wound from gunshot or stab wound
- Deficits:
- Ipsilateral loss of two-point discrimination, pressure, vibration, and proprioception (dorsal column lateral meniscus)
- Ipsilateral loss of motor function (corticospinal tract)
- Contralateral loss of pain and temperature (spinothalamic)
- Intact: None
- Posterior cord syndrome
- Etiology: Cervical hyperextension
- Deficits:
- Bilateral loss of proprioception, vibration, and pressure (dorsal column lateral meniscus)
- Intact:
- Preservation of motor function (corticospinal)
- Pain and temperature (spinothalamic)
- Cauda equina injury (classified as lower motor neuron lesion)
- Etiology: Trauma, herniated disk, spinal stenosis, infections below the L1 nerve root
- Deficits:
- Flaccid paralysis of bladder, bowel function (incontinence)
- Impaired motor function — specifically lower extremities
- Absent spinal reflexes
- Intact: Variable dependent upon the severity of injury
Associated disorders with spinal cord injury
- Spinal shock:
- Immediately after injury a time of absent reflexes and flaccidity due to the body working to protect itself after injury
- Timeframe can vary from 24 hours to 24 weeks
- Difficult to get an accurate ASIA assessment due to spinal shock and changes in the level of injury
- Autonomic dysreflexia
- Medical emergency for individuals with T6 or above injury
- Caused by noxious stimuli in individuals with spinal cord injury who are unable to regulate sympathetic responses below the level of injury.
- Noxious stimulus causes activation of the sympathetic nervous system, and due to spinal cord injury, the parasympathetic nervous system is unable to be activated due to injury to the spinal cord (activation of the parasympathetic system will cancel out the effects of the sympathetic nervous system
- Noxious stimuli can be constipation, catheter malfunction, pressure injuries, tight clothes, or sitting on a sharp object
- Noxious stimulus causes activation of the sympathetic nervous system, and due to spinal cord injury, the parasympathetic nervous system is unable to be activated due to injury to the spinal cord (activation of the parasympathetic system will cancel out the effects of the sympathetic nervous system
- Symptoms: headache, increased blood pressure, bradycardia, diaphoresis above the level of injury, flushing below the level of injury, seizures. If left untreated, it can lead to death.
- Medical management: sit the patient up and assess for noxious stimulus
- Spasticity
- Increased tone to extremities or trunk due to consistent contraction; leads to range of motion deficits and functional impairment
- Will only be seen in upper motor neuron lesions
- Occurs most often in incomplete lesions
- Utilize the Modified Ashworth Scale to assess
- Heterotopic ossification
- Abnormal bone growth in the muscle
- Symptoms: firmness at the muscle site, pain with palpation, pain with muscle stretch or palpation
- Typically involves the quadriceps and brachialis muscles
- Deep vein thrombosis:
- Medical emergency
- Development due to immobility of extremities, which places individuals at increased risk for blood clot development
- Treatment option: graduated compression socks, anti-coagulation medication
Levels of independence (for complete injuries)
- Transfers
- C1-C5: dependent transfers
- C6: independent with sliding board transfers on level surfaces
- C7 and beyond: independent with transfers without a sliding board on unlevel surfaces
- Wheelchair use
- C1-C5: power wheelchair use with the use of head control, mouth control, or joystick
- C6: manual wheelchair on level surfaces with use of wheel projections and large knobby wheels- independent status
- C7 and beyond: manual wheelchair usage without adaptations on all surfaces- independent status
- Gait
- T12:
- Exercise only ambulation due to high energy needs
- Hip-knee-ankle orthosis (HKAFO) with the hip locked in extension or a reciprocating gait orthosis (RGO) is necessary for gait
- Manual wheelchair used primarily
- L1-L2:
- Exercise only ambulation due to high energy needs
- Hip-knee-ankle orthosis with the hip unlocked to allow for flexion to occur, necessary for ambulation
- Manual wheelchair used primarily
- L3:
- Household ambulation
- Ankle foot orthosis (AFO) used to assist with knee control
- Manual wheelchair used for community mobility
- L4 and below:
- Community ambulation
- Ankle foot orthosis (AFO) used to assist with ankle control
- Manual wheelchair used as needed
- T12:
Parkinson’s disease
Common impairments of Parkinson’s disease
- Resting tremor
- Impaired postural reflexes
- Cogwheel rigidity
- Bradykinesia
- Slowed reaction time
- Masked face
- Dysarthria
- Hypophonia (decreased speech volume)
- Contractures in the flexor and adductor muscles
- Postural deficits- rounded shoulders, kyphosis
- Restrictive lung disease
- Visual impairment
- Dementia in later stages
Standardized test for Parkinson’s disease
Hoehn & Yahr classification of disability
Stage 1
- Disability: Minimal or absent
- Extent of disability: Unilateral
Stage 2
- Disability: Minimal
- Extent of disability: Midline involvement and bilateral
Stage 3
- Disability: Impaired postural reflexes, unsteadiness when rising from a chair; continues to be independent and work
- Extent of disability: Midline involvement and bilateral
Stage 4
- Disability: All symptoms present; ambulation only with assistive device
- Extent of disability: Midline involvement and bilateral
Stage 5
- Disability: All symptoms present; confined to wheelchair or bed
- Extent of disability: Midline involvement and bilateral
Retropulsion pull test
Testing Procedures:
- The subject stands in a comfortable stance with eyes open (have feet shoulder width apart if they assume an unusually wide or narrow stance).
- The examiner stands behind the subject.
- The subject is instructed to do whatever it takes not to fall and is told that the examiner will catch them if they do fall.
- The examiner gives a sudden, brief backward pull to the shoulders with sufficient force to cause the subject to have to regain their balance.
- The subject should not know exactly when the pull is coming.
Interpretation of results: scoring is from 0 to 4:
- 0 = recovers independently, may take 1 or 2 steps or an ankle reaction
- 1 = three steps or more backward, but recovers independently
- 2 = retropulsion, needs to be assisted to prevent a fall
- 3 = very unstable, tends to lose balance spontaneously
- 4 = unable to stand without assistance (UPDRS method)
Medication for Parkinson’s disease
- Levodopa
- Mechanism of action: relieve symptoms of Parkinson’s disease by turning levodopa into dopamine (due to a lack of dopamine in the basal ganglia)
- Side effects: mental confusion, hallucinations, postural hypotension, restlessness, abnormal movements
- On and off time: Levodopa should be given 1 hour before initiation of activity for optimal effects; medication will wear off , and symptoms will occur
- Anticholinergic medications
- Mechanism of action: decreases tremors by blocking cholinergic production in the asal ganglia
- Side effects: dry mouth, urine retention, constipation
Huntington’s disease
Symptoms
- Involuntary writhing movements (choreic movements) at rest
- Muscle rigidity
- Poor balance
- Difficulty with swallowing/speaking
- Impaired executive function
- Decline in overall mental health
- Functional decline
Physical therapy considerations with Huntington’s disease
- Balance/gait exercise- using a weighted walker
- Postural stability
- Family education/training as needed
- No modalities indicated
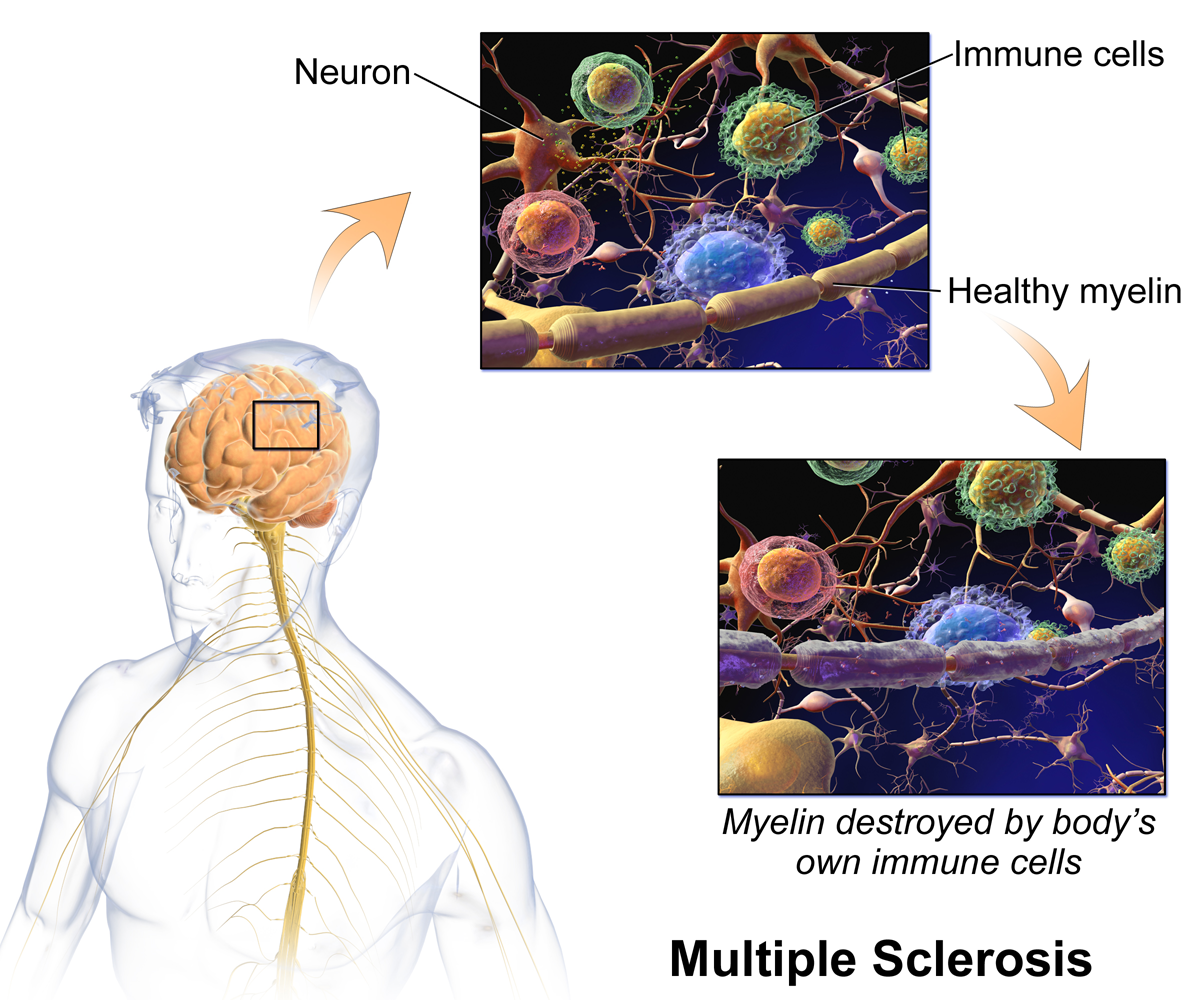
Multiple sclerosis (MS)
Types of Multiple Sclerosis
- Relapsing-remitting
- Characterized by cycles of disease exacerbation followed by periods of remission; varied levels of disability
- Primary progressive
- Characterized by disease consistently being present without remission; permanent disability results
- Secondary-progressive
- Characterized by disease beginning as cyclic relapse/remitting initially, followed by continuous progression of disease without remission; permanent disability results
- Progressive-relapsing
- Characterized by progressive disease with unpredictable times of remission; permanent disability results
Symptoms of multiple sclerosis- symptoms will vary depending on the location of plaques
- Weakness
- Spasticity
- Hyperreflexia
- Impaired coordination
- Visual deficits
- Ataxia
- Vestibular dysfunction
- Dysarthria
- Paresthesia
- Lhermitte’s sign: electric shock-like symptoms resulting from neck flexion
Special considerations with multiple sclerosis
- Avoidance of precipitating factors:
- Stress
- Trauma
- Pregnancy
- Trauma
- Heat
- Hyperventilation
- Dehydration
- Increase exertion
Amyotrophic lateral sclerosis (ALS)
Symptoms
- Asymmetrical weakness
- Facial weakness
- Difficulty with swallowing
- Hyperreflexia
- Spasticity
- Compromised cranial nerve integrity
Stages of ALS
Stage 1- early stage
- Mild weakness or stiffness in the hands, feet, or limbs
- May have difficulty with fine motor tasks (e.g., writing, buttoning)
Stage 2- middle severe
- Weakness spreads to other parts of the body
- Difficulty walking, speaking, or swallowing
- May require assistance with daily activities
Stage 3 — late state severe:
- Late Stage: Severe weakness and paralysis, Difficulty breathing, and need for a wheelchair and ventilator.
Stage 4- end stage
- Total paralysis
- Loss of cognitive function in some cases may occur, but rare
Medical management is the treatment of symptoms, as there is no cure for ALS. Motor function progressively diminishes until the individual becomes totally dependent for activities of daily living and mobility while on ventilator support. Physical therapy assists with the prescription of assistive devices and family education/training as appropriate.
Epilepsy
Symptoms:
- Altered consciousness
- Convulsions
- Sensory phenomena: heightened somatosensory, visual, auditory, or olfactory senses
- Autonomic phenomena: tachycardia, anxiety, diaphoresis
- Cognitive phenomena: inability to communicate, hallucinations
Classification of epilepsy
- Generalized
- Involves all areas of the brain
- Symptoms include loss of consciousness, rhythmic movements of extremities (convulsions), loss of bladder function, and alterations in breathing
- Lasting 1-5 minutes
- Absent
- Typically, no symptoms are present, which increases the difficulty of diagnosing the condition
- Repetitive blinking or small movements may be present
- Last for seconds and can occur multiple times per day
- Typically, no symptoms are present, which increases the difficulty of diagnosing the condition
- Partial or focal
- Only one part of the brain is involved, which causes symptoms to be focal
- Status epilepticus
- Prolonged seizures or a series of seizures with only brief moments of recovery
- Lasting 30 minutes or longer
Physical therapy and epilepsy
- To do if a seizure occurs
- Protect the airway
- Roll to sidelying
- Loosen restrictive clothes
- Remove harmful objects that may be nearby
- Do not restrain limbs
- Seek medical attention immediately at the conclusion of convulsions