
Heart failure
Heart failure (cardiac failure) is the inability of the heart to maintain an adequate cardiac output to meet the body’s metabolic needs. It can be:
- Systolic or diastolic
- Left ventricular, right ventricular, or biventricular
- Acute or chronic
Systolic failure is failure of the ventricle’s normal pumping ability. It presents with a reduced ejection fraction (EF) (<40%).
Diastolic dysfunction is impaired ventricular relaxation or filling due to increased wall stiffness. EF is preserved in diastolic dysfunction, but filling pressures are increased.
Congestive heart failure is heart failure with pulmonary and/or systemic congestion. It can occur in LHF, RHF, or biventricular failure.
Common causes of heart failure
- CAD or IHD
- DM
- Hypertension
- Cardiomyopathy
- Myocarditis
- Congenital heart disease
- Valvular heart disease
- Arrhythmias esp. tachyarrhythmias
- Alcohol abuse, Beriberi
- HIV/AIDS
- Hypervitaminosis E
- Radiation or chemotherapy
- Thyroid disorders
- Severe anemia
- Cocaine and drug abuse
- AV shunts
- Massive pulmonary embolism
- Cardiac tamponade and constrictive pericarditis
I) Left-sided heart failure (LHF):
LHF results from left ventricular (LV) dysfunction.
- Systolic dysfunction of the LV is due to impaired ventricular contractility. Causes include AMI, CAD, volume overload from MR or AR, and dilated cardiomyopathy.
- Systolic dysfunction can also result from increased afterload, such as systemic hypertension or aortic stenosis.
- Diastolic dysfunction of the LV is due to impaired relaxation (for example, from LVH, HOCM, restrictive cardiomyopathy, or CAD) or impaired ventricular filling (for example, from MS, cardiac tamponade, or constrictive pericarditis).
LHF causes fluid accumulation in the lungs (pulmonary edema) and systemic hypoperfusion.
II) Right-sided heart failure (RHF):
RHF results from right ventricular (RV) dysfunction.
- Systolic dysfunction of the RV may result from increased afterload due to pulmonary HT, COPD, PE, ILD, ARDS, or pulmonic stenosis.
- Impaired RV contractility can also result from AMI, volume overload from TR or PR, and dilated cardiomyopathy.
- Diastolic dysfunction of the RV can result from tricuspid stenosis, plus pathologies similar to those causing diastolic dysfunction of the LV (such as tamponade).
The most common cause of RV failure is LV failure. RHF causes fluid buildup in the systemic and portal venous system, presenting as peripheral pitting edema and hepatic congestion.
Comparison between LHF and RHF
LHF
- Dyspnea, orthopnea, paroxysmal nocturnal dyspnea
- Cough with frothy sputum
- Decreased urine output
- Pulmonary crackles, rhonchi
- In severe cases, loud P2, systolic murmur from MR, pulsus alternans
- Hemosiderin containing alveolar macrophages or “heart failure” cells
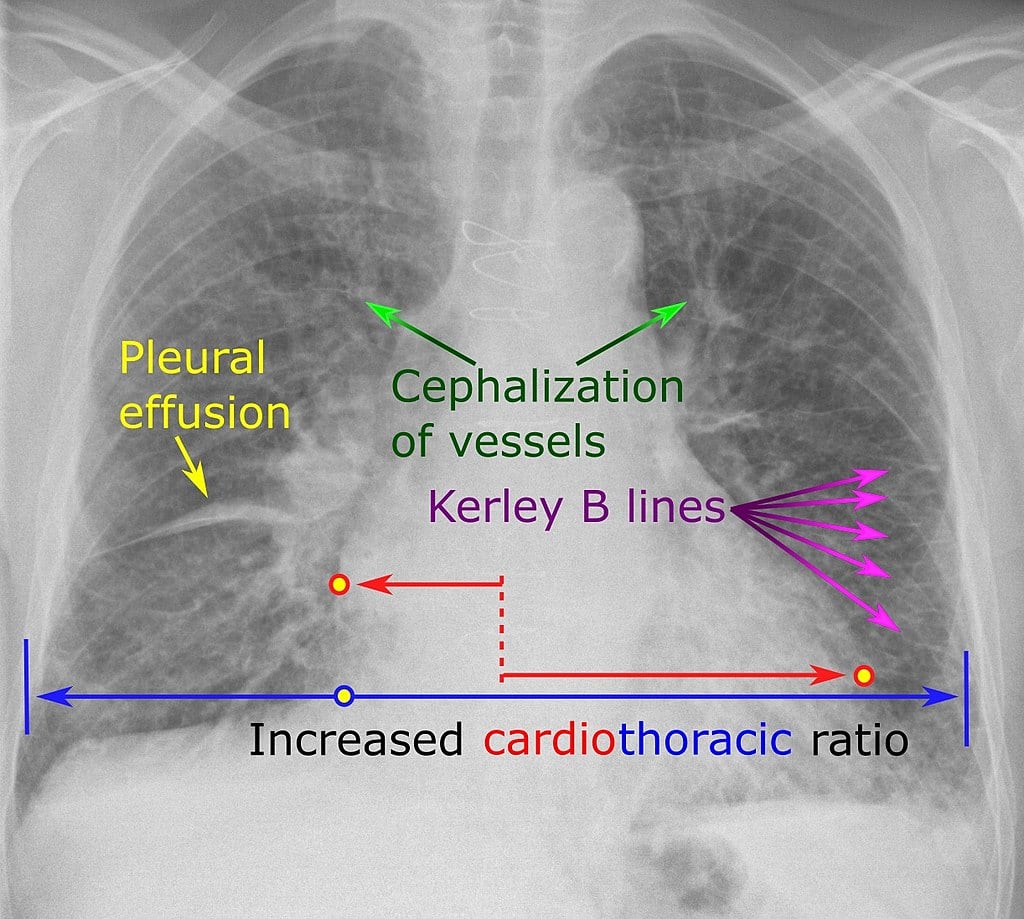
- CxR shows Kerley’s B lines on from septal pulmonary edema; perihilar congestion and alveolar infiltrates
RHF
- Peripheral pitting edema, ascitis
- Hepatosplenomegaly
- Raised JVP
- In severe cases, Kussmaul sign, TR murmur and right ventricular heave
- Hepatojugular reflex will be positive
- Central cyanosis more common
S3 and S4 can be auscultated.
- S3 is due to abnormal filling of blood into an already volume-overloaded ventricle.
- S4 is due to forceful atrial contraction against a stiff ventricle and is seen in diastolic dysfunction such as LVH or RVH.