Integumentary system
Foundational skin information
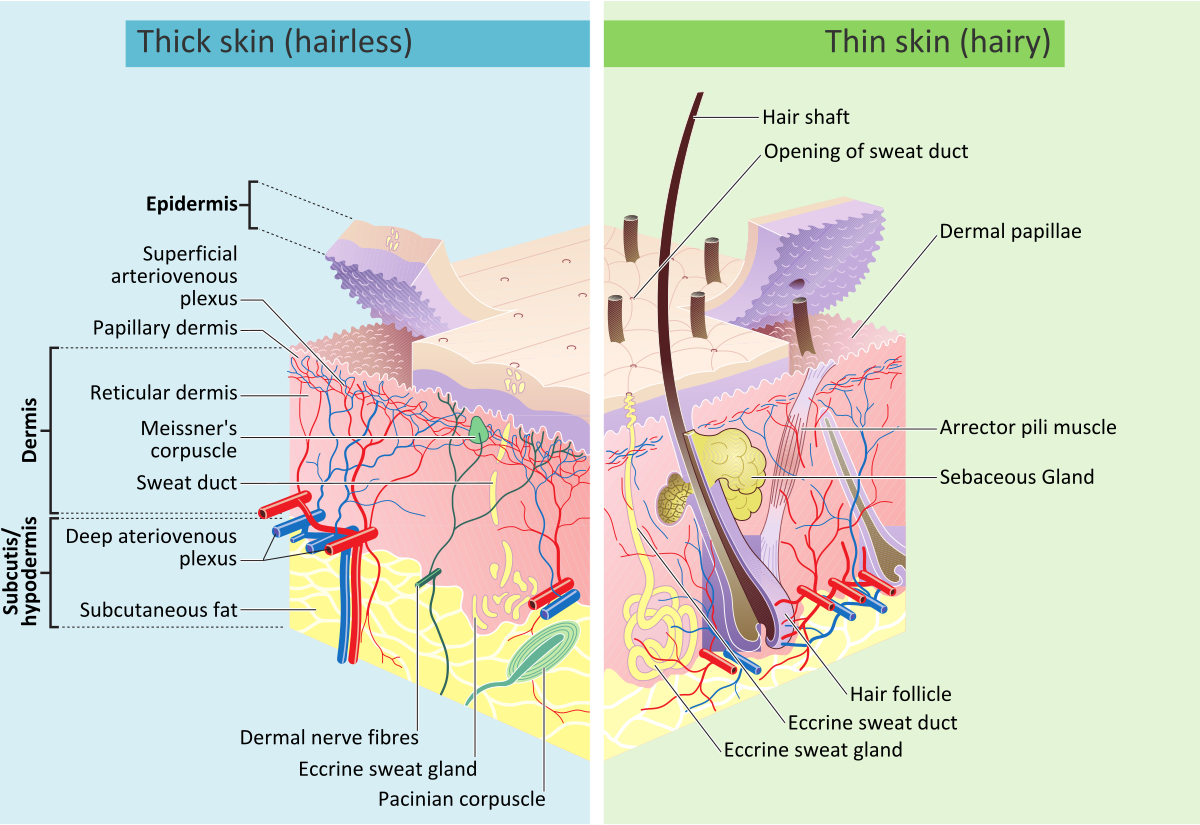
Epidermis (outermost layer)
- Avascular (no blood vessels)
- Composed of keratinized stratified squamous epithelium
- Key Cells:
- Keratinocytes — Strength and waterproofing (keratin production)
- Melanocytes — Pigmentation and ultraviolet light protection
- Langerhans cells — Immune defense
- Merkel cells — Touch sensation
- Epidermal layers (Deep → Superficial)
- Stratum basale (Germinativum) — Active mitosis, melanocytes present
- Stratum spinosum — Thickest layer, desmosomes for strength
- Stratum granulosum — Keratinization begins
- Stratum lucidum — Only in thick skin (palms/soles)
- Stratum corneum — Dead keratinized cells (barrier layer)
Dermis (middle layer)
- Vascularized, supplies nutrients to the epidermis
- Contains:
- Blood vessels
- Nerve endings
- Hair follicles
- Sweat and sebaceous glands
- Collagen and elastin fibers (structural support)
- Dermal layers:
- Papillary layer — loose connective tissue, fingerprints, touch receptors
- Reticular layer — dense, irregular connective tissue, deep pressure receptors
Hypodermis (subcutaneous tissue — deepest layer)
- Composed of: fat (adipose tissue), connective tissue
- Function: insulation, energy storage, shock absorption
Related to skin
- Hair — protects against UV, insulates scalp
- Nails — keratinized structures for protection and dexterity
- Sebaceous (Oil) glands — secrete sebum (moisturizes and protects skin)
- Sweat glands — regulate temperature and remove waste
- Eccrine glands — watery sweat, found everywhere
Wound healing phases
Inflammatory phase
- Initiated immediately and lasts 3-4 days
- Marked by hemostasis (stopping bleeding) and phagocytosis (removal of debris and pathogens)
Proliferative phase
- Lasts until day 21 post-injury
- Collagen formation: A whitish protein substance that adds to the tensile strength of the wound
- Eschar formation may occur
Maturation phase
- Begins at day 21 and lasts up to 1-2 years
- Leads to scar formation
Types of healing
Primary intention (first intention)
- Tissue surfaces are closed with minimal tissue loss
- Example: Surgical incision
Secondary intention
- Extensive tissue loss prevents edges from being approximated
- Example: Pressure ulcer
- Longer repair time, increased scarring, and higher infection risk
Tertiary intention healing (delayed closure)
- Wound is left open for a period before closure
- Example: Abdominal wound left open for drainage before later closure
Classification of wound drainage
- Serous — Clear to brownish fluid from the serum portion of blood
- Sanguineous — Bright red, bloody drainage
- Serosanguineous — Pinkish drainage, a mix of blood and serum
- Purulent — Thick, yellow or yellow-green pus, indicating infection
How to measure wounds accurately
Tools needed for wound measurement
- Disposable ruler (centimeters or millimeters)
- Sterile cotton-tipped applicator (for depth)
- Wound probe (for tunneling or undermining)
- Gloves (to maintain infection control)
- Transparent film grid (optional for tracing irregular shapes)
Step-by-step wound measurement
Measuring length and width
- Patient positioning: Ensure the patient is in the same position each time for consistency
- Use a ruler: Place a disposable ruler over the wound
- Length measurement: Measure from the longest point head-to-toe (cephalad to caudal)
- Width measurement: Measure perpendicular to the length, at the widest point from side to side
- Documentation format: Length × Width (e.g., 5.2 cm × 3.4 cm)
Measuring wound depth
- Insert a sterile cotton-tipped applicator into the deepest part of the wound
- Mark the level where it meets the wound edge (this should be perpendicular to the cotton applicator)
- Remove and measure against a ruler
- Example documentation: Depth = 0.8 cm
Measuring wound volume
- Measuring wound volume can be done by multiplying length, width, and depth
- Measure the amount of hydrogel required to fill the wound
Steps for measuring tunneling and undermining
- Insert a sterile probe into the suspected tunnel/undermined area
- Measure using a ruler
- Use the clock method to describe location (e.g., “Tunneling at 3 o’clock position, depth 1.5 cm”)
Additional documentation details
- Shape and edges: Irregular, round, oval, jagged
- Tissue type: Granulation, slough, eschar
- Exudate: amount (none, scant, moderate, heavy) and type (serous, purulent, sanguineous)
- Periwound skin: Erythema, edema, maceration, induration
Types of dressing
Gauze dressings
- Names: Sterile gauze, non-sterile gauze, impregnated gauze
- Indications: Used for wounds with moderate to heavy exudate, surgical wounds, and packing deep wounds, and pressure injuries stages III, IV.
- Contraindications: Not ideal for dry wounds (can cause adherence and delay healing)
Transparent film dressings
- Names: Tegaderm, Opsite, Bioclusive
- Indications: Superficial wounds, abrasions, and partial-thickness wounds with minimal exudate; also used for IV sites; used for IV sites, and pressure injuries stages I, II.
- Contraindications: Should not be used on heavily exudating wounds or infected wounds
Hydrocolloid dressings
- Names: Duoderm, Comfeel, Tegasorb
- Indications: Moderate exudating wounds, pressure injuries stages II, III, IV and venous leg ulcers. Helps maintain a moist wound environment.
- Contraindications: Not suitable for infected wounds or wounds with heavy exudate.
Hydrogel dressings
- Names: IntraSite Gel, Aquaform, Vigilon
- Types: Gel, sheet, or beads (for deep wounds)
- Indications: Dry wounds, burns, painful wounds, and wounds with necrotic tissue (autolytic debridement), and pressure injuries stages II, III, IV.
- Contraindications: Should not be used on heavily exudating wounds as it can cause maceration.
Foam dressings
- Names: Allevyn, Mepilex, Lyofoam
- Indications: Moderate to heavily exudating wounds, venous ulcers, pressure ulcers, and diabetic foot ulcers and pressure injuries stages II, III, IV. Provides cushioning.
- Contraindications: Not ideal for dry wounds or wounds with minimal exudate.
Alginate dressings
- Names: Kaltostat, Sorbsan, Algicell
- Indications: Heavy exudating wounds, infected wounds, and wounds with tunneling. Derived from seaweed, absorbs large amounts of fluid, and pressure injuries stages III, IV.
- Contraindications: Not recommended for dry wounds or wounds with minimal exudate.
- Characteristics: When an alginate dressing is removed, it can have a yellowish, tan, or brown color and may have a mild, but unpleasant odor. While the appearance and smell can be alarming, they are often normal and result from the interaction between the seaweed-based dressing and the wound’s exudate.
Collagen dressings
- Names: Promogran, Fibracol, Biostep
- Indications: Chronic non-healing wounds, pressure ulcers, wounds with granulation tissue, and pressure injuries stages II, III, IV.
- Encourages new tissue growth.
- Contraindications: Not for dry wounds or wounds with eschar. Avoid in patients with collagen allergies.
Antimicrobial dressings
- Names: Silvercel, Acticoat, Iodosorb
- Indications: Infected wounds, burns, surgical wounds at risk of infection, and pressure injuries stages II, III, IV. Contains silver or iodine to reduce bacterial load.
- Contraindications: Avoid in patients allergic to silver or iodine. Not recommended for long-term use due to potential cytotoxicity.
Types of debridement
Autolytic debridement
- Definition: Uses the body’s own enzymes and moisture to break down necrotic tissue.
- Methods: Hydrocolloid, hydrogel, or transparent film dressings.
- Indications:
- Wounds with necrotic tissue (eschar or slough).
- Patients who cannot tolerate more aggressive debridement.
- Minimal to moderate exudating wounds.
- Contraindications:
- Infected wounds.
- Heavily exudating wounds.
Mechanical debridement
- Definition: Uses physical forces to remove necrotic tissue.
- Methods:
- Wet-to-dry dressings (gauze applied wet and removed dry).
- Hydrotherapy (whirlpool).
- Pulsed lavage (pressurized irrigation).
- Indications:
- Moderate to heavily necrotic wounds.
- Wounds with thick, adherent slough or debris.
- Contraindications:
- Painful wounds.
- Granulating wounds (can damage healthy tissue).
Enzymatic debridement
- Definition: Uses topical enzymatic agents to break down necrotic tissue.
- Methods: Application of collagenase (e.g., Santyl).
- Indications:
- Wounds with thick, adherent necrotic tissue.
- Patients unable to tolerate surgical or sharp debridement.
- Contraindications:
- Infected wounds without antibiotic coverage.
- Clean wounds with no necrotic tissue.
Sharp debridement
- Definition: Uses scalpels, scissors, or forceps to remove necrotic tissue manually.
- Indications:
- Wounds with extensive necrosis or thick eschar.
- Infected wounds requiring immediate removal of necrotic tissue.
- Contraindications:
- Bleeding disorders or anticoagulated patients.
- Poor vascular supply (risk of delayed healing).
Surgical debridement
- Definition: Performed by a surgeon in an operating room to remove large amounts of necrotic tissue.
- Indications:
- Deep wounds with extensive necrosis.
- Life-threatening infections (e.g., necrotizing fasciitis).
- Chronic non-healing wounds requiring aggressive intervention.
- Contraindications:
- Patients who are medically unstable for surgery.
Biological (maggot) debridement
- Definition: Uses sterile maggots (larvae of Lucilia sericata) to digest necrotic tissue and bacteria.
- Indications:
- Chronic, non-healing wounds with necrotic tissue.
- Infected wounds (maggots secrete antimicrobial enzymes).
- Contraindications:
- Patient refusal.
- Allergies to fly larvae or materials used in dressing containment.
Wound classifications by etiology
Arterial wounds
Cause: Reduced arterial blood supply leading to ischemia and necrosis.
Characteristics:
- Location: Toes, lateral malleolus, dorsum of the foot, distal lower extremities.
- Appearance: Punched-out, deep with well-defined edges.
- Wound Bed: Pale, necrotic, minimal granulation tissue.
- Drainage: Minimal (often dry).
- Surrounding Skin: Cool, shiny, thin, hair loss, pallor with elevation, dependent rubor.
- Pain: Severe, worsens with elevation, relieved in a dependent position.
- Pulses: Diminished or absent.
- Risk Factors: Peripheral arterial disease (PAD), smoking, diabetes, and hypertension.
Grading
- Partial thickness — depth only extends through the epidermis and parts of the dermis
- Full thickness — depth extends to subcutaneous tissue
Venous wounds
Cause: Venous insufficiency leading to fluid retention, inflammation, and skin breakdown.
Characteristics:
- Location: Medial malleolus, lower leg (gaiter region).
- Appearance: Shallow, irregular borders, large wound area.
- Wound Bed: Granular, red with yellow fibrinous tissue.
- Drainage: Moderate to heavy (wet wound)
- Surrounding Skin: Edema, hemosiderin staining (brown discoloration), lipodermatosclerosis (thickened skin).
- Pain: Mild to moderate, relieved by elevation.
- Pulses: Present but may be difficult to palpate due to edema.
- Risk Factors: Chronic venous insufficiency, varicose veins, obesity, prolonged standing.
Grading
- Partial thickness — depth only extends through the epidermis and parts of the dermis
- Full thickness — depth extends to subcutaneous tissue
Pressure wounds
Cause: Prolonged pressure, shear, or friction leading to ischemic damage.
Characteristics:
- Location: Bony prominences (sacrum, heels, ischial tuberosities, greater trochanter).
- Appearance: Varies by stage, from non-blanchable redness to deep tissue damage.
- Drainage: Variable (depends on stage and infection presence).
- Surrounding Skin: May show maceration, erythema, or induration.
- Pain: Variable (more in early stages, less in advanced necrotic ulcers).
- Risk Factors: Immobility, malnutrition, incontinence, neuropathy.**
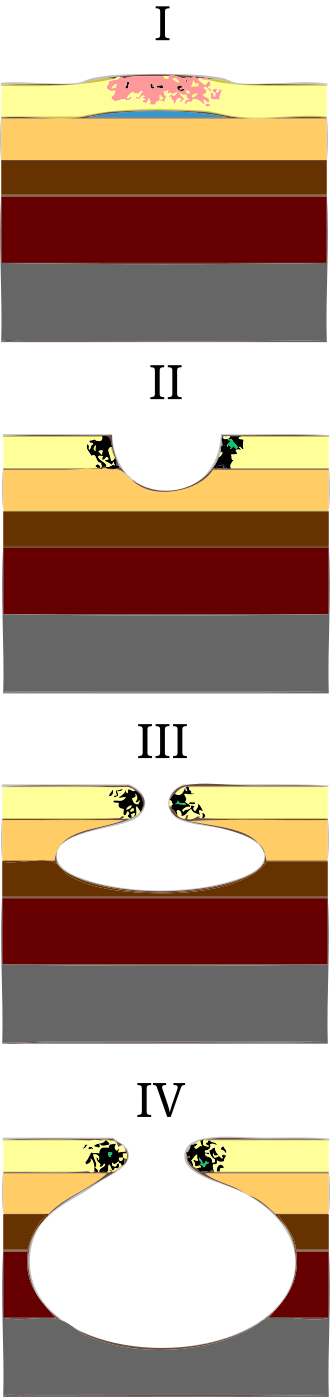
Grading: national pressure injury staging
- Stage 1: Non-blanchable erythema, intact skin.
- Stage 2: Partial-thickness skin loss (blister or shallow ulcer).
- Stage 3: Full-thickness skin loss with visible fat, but no bone/muscle.
- Stage 4: Full-thickness with exposed bone, muscle, or tendon.
- Unstageable: Wound covered by necrotic tissue, depth unclear.
- Deep tissue injury: Intact or non-intact skin with persistent non-blanchable deep red, maroon, or purple discoloration.
Diabetic wounds
Cause: Peripheral neuropathy, pressure, and poor circulation due to diabetes.
Characteristics:
- Location: Plantar surface of foot, metatarsal heads, heels, toes.
- Appearance: Punched-out, round, deep, with well-defined edges.
- Wound Bed: Pale or granulating tissue, may have necrosis.
- Drainage: Minimal unless infected.
- Surrounding Skin: Calloused, dry, cracked, loss of protective sensation (neuropathy).
- Pain: Typically painless due to neuropathy.
- Pulses: May be present or diminished (if arterial disease is also present).
- Risk Factors: Diabetes, poor glycemic control, loss of sensation, and foot deformities.
Grading: Wagner classification for diabetic foot ulcers
- Grade 0: Intact skin with high risk (calluses, foot deformities).
- Grade 1: Superficial ulcer (partial/full-thickness skin loss).
- Grade 2: Ulcer extending to tendon, bone, or capsule.
- Grade 3: Deep ulcer with abscess, osteomyelitis.
- Grade 4: Localized gangrene.
- Grade 5: Extensive gangrene of the foot requiring amputation.
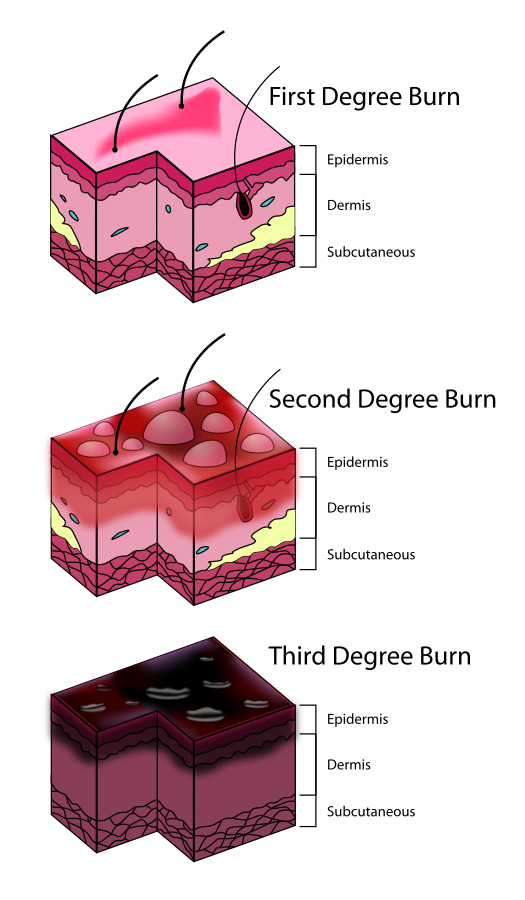
Burns
Causes: Thermal, friction, electrical, chemical, radiation
The presentation of burns is determined by the classification. See below:
Superficial (First-degree burn)
- Layers Affected: Epidermis only
- Appearance: Red, dry, no blisters
- Pain Level: Mild to moderate
- Healing Time: 3-7 days without scarring
- Example: Sunburn
Partial-thickness (second-degree burn)
a. Superficial Partial-Thickness
- Layers Affected: Epidermis + upper dermis
- Appearance: Red, moist, blisters present
- Pain Level: Very painful (nerve endings intact)
- Healing Time: 10-21 days, minimal to no scarring
b. Deep Partial-Thickness
- Layers Affected: Epidermis + deeper dermis
- Appearance: Mottled red/white, sluggish blanching
- Pain Level: Less painful (nerve endings damaged)
- Healing Time: 3-6 weeks, scarring likely
Full-Thickness (third-degree burn)
- Layers Affected: Epidermis + entire dermis (may extend to subcutaneous tissue)
- Appearance: White, leathery, charred, dry
- Pain Level: Painless (nerve endings destroyed)
- Healing Time: Requires skin grafting, significant scarring
Subdermal (fourth-degree burn)
- Layers Affected: Epidermis, dermis, fat, muscle, and bone
- Appearance: Black, charred, necrotic tissue
- Pain Level: Painless (complete nerve destruction)
- Healing Time: Requires surgical intervention; amputation is possible
Use of grafts for burns
- Autografts: taken from the individual
- Allografts: taken from cadavers
- Xenografts: taken from another species (i.e, pig, cow)
Interventions for burns
First-degree burns
- Cool the burn with cool water.
- Apply over-the-counter pain relievers, such as NSAIDs or acetaminophen.
- Use aloe vera gel or petroleum jelly to soothe the burn.
Second-degree burns
- In addition to the above, apply a topical antibiotic cream, such as Bacitracin or Neomycin.
- Cover the burn with a non-stick dressing.
- Use silver sulfadiazine cream to prevent infection.
Third-degree burns
- Intravenous fluids and pain relievers
- Antibiotic therapy
- Topical dressings, such as mafenide acetate or silver sulfadiazine
- Surgery may be necessary to remove the burned skin and graft new skin.
Other medications
- Corticosteroids may be used to reduce inflammation.
- Antihistamines may be used to relieve itching.
- Sedatives may be used to manage pain and anxiety.
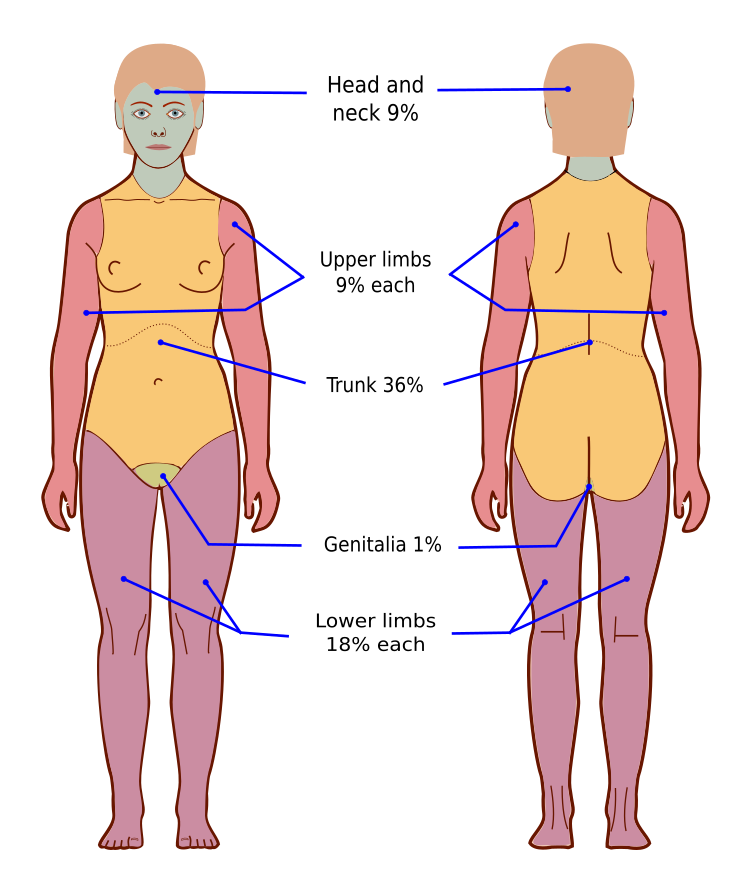
Rule of Nines for burn assessment
The Rule of Nines is a quick method to estimate the total body surface area (TBSA) affected by burns. It differs for adults and children due to variations in body proportions.
Rule of Nines for adults
Rule of Nines for children
Other common skin conditions
Impetigo
Impetigo is a bacterial skin infection caused by Staphylococcus aureus or Streptococcus pyogenes. It is highly contagious and commonly affects children. The hallmark feature is honey-colored, crusted lesions that typically appear around the mouth, nose, and hands. Mild itching may be present, but systemic symptoms like fever are rare. Since impetigo is superficial, it does not cause deep tissue damage and is easily treatable with antibiotics.
Cellulitis
Cellulitis is a bacterial skin infection that occurs in the deeper layers of the skin and subcutaneous tissue. It is most commonly caused by Staphylococcus aureus or Streptococcus pyogenes. Unlike impetigo, cellulitis presents with diffuse redness, warmth, swelling, and pain, and it may be accompanied by systemic symptoms such as fever, chills, and malaise. It commonly affects the lower extremities, but can occur anywhere. Cellulitis can spread quickly and requires antibiotics, and in severe cases, hospitalization may be necessary.
Herpes Zoster (Shingles)
Herpes zoster, or shingles, is a viral infection caused by the reactivation of the varicella-zoster virus (the same virus that causes chickenpox). It presents as a painful, blistering rash that follows a dermatomal pattern—meaning it is limited to one side of the body along a nerve path. Before the rash appears, individuals may experience burning, tingling, or flu-like symptoms. Unlike impetigo and cellulitis, herpes zoster is not a bacterial infection and requires antiviral treatment. A significant complication is post-herpetic neuralgia, which can cause chronic nerve pain even after the rash has resolved.
Dermatitis (Eczema)
Dermatitis is a non-infectious inflammatory skin condition caused by an immune response to allergens, irritants, or chronic skin sensitivity. It presents as red, dry, scaly, and itchy skin and is often associated with pruritus (intense itching). Unlike the other conditions, dermatitis is not contagious and does not involve bacterial or viral pathogens. Common triggers include allergens, soaps, stress, and climate changes. Treatment involves moisturizers, corticosteroids, and avoiding triggers.
Psoriasis
Psoriasis is a chronic autoimmune skin condition that causes rapid skin cell turnover, leading to the buildup of thick, scaly plaques on the skin. It is characterized by red, inflamed patches with silvery-white scales, often appearing on the scalp, elbows, knees, and lower back. The condition is not contagious and can be triggered by stress, infections, medications, and environmental factors. Psoriasis is associated with immune system dysfunction, specifically involving T-cells and inflammatory cytokines. It can also be linked to psoriatic arthritis, which affects the joints. Treatment includes topical steroids, phototherapy, and systemic immunosuppressants.
Sclerederma
Scleroderma is a chronic autoimmune connective tissue disease characterized by abnormal collagen deposition, leading to skin thickening, fibrosis, and vascular dysfunction. It can affect the skin, blood vessels, and internal organs, including the lungs, heart, kidneys, and gastrointestinal tract.
There are two main types:
1. Localized Scleroderma — Primarily affects the skin and underlying tissues, often in morphea or linear forms.
2. Systemic Sclerosis (Systemic Scleroderma) — Involves widespread fibrosis affecting the skin and internal organs.
Common symptoms include tight, hard skin, Raynaud’s phenomenon, joint pain, and digestive issues. The exact cause is unknown, but it is believed to involve immune system dysfunction and genetic/environmental factors. There is no cure, but treatment focuses on managing symptoms and slowing disease progression with immunosuppressants, vasodilators, and physical therapy.