Gastrointestinal, reproductive and renal system
Common gastrointestinal tests
Gastroesophageal reflux disease (GERD)
- Description: Backflow of stomach acid into the esophagus due to a weakened lower esophageal sphincter
- Symptoms: Heartburn, regurgitation, chest pain, difficulty swallowing
- PT implications: Avoid exercises that increase intra-abdominal pressure; encourage upright positions after eating
Peptic ulcer disease (PUD)
- Description: Open sores in the stomach or duodenal lining, often caused by H. pylori infection or NSAIDs
- Symptoms: Epigastric pain, nausea, bloating, bloody stool (if severe)
- PT implications: Monitor for signs of GI bleeding (dark stool, fatigue, pallor)
Irritable bowel syndrome (IBS)
- Description: Functional GI disorder with chronic abdominal pain and altered bowel habits (diarrhea, constipation, or both)
- Symptoms: Cramping, bloating, diarrhea, constipation, mucus in stool
- PT implications: Stress management, exercise to regulate bowel motility
Crohn’s disease
- Description: Chronic inflammation of any part of the GI tract, often the small intestine
- Symptoms: Abdominal pain, diarrhea, weight loss, fatigue, malnutrition
- PT implications: Address fatigue, joint pain, and osteoporosis risks due to long-term steroid usage for disease management.
Ulcerative colitis
- Description: Chronic inflammation and ulcers in the colon and rectum
- Symptoms: Bloody diarrhea, urgency, abdominal cramping, weight loss
- PT implications: Monitor for dehydration, anemia, and musculoskeletal complications
Diverticulitis
- Description: Infection or inflammation of diverticula (pouches in the colon wall)
- Symptoms: Lower left quadrant pain, fever, nausea, bowel habit changes
- PT implications: Avoid increased intra-abdominal pressure (e.g., Valsalva maneuver)
Celiac disease
- Description: Autoimmune disorder triggered by gluten, leading to villous atrophy in the small intestine
- Symptoms: Malabsorption, diarrhea, bloating, fatigue, weight loss
- PT implications: Monitor for signs of malnutrition, osteoporosis, and neurological symptoms (tingling, numbness)
Hepatitis (A, B, C, D, E)
- Description: Inflammation of the liver, often viral
- Symptoms: Jaundice, fatigue, dark urine, nausea, right upper quadrant pain
- PT implications: Energy conservation techniques, avoid strenuous exercise during active infection
Cirrhosis
- Description: Chronic liver disease with fibrosis and impaired liver function
- Symptoms: Jaundice, ascites, hepatomegaly, fatigue, confusion (hepatic encephalopathy)
- PT implications: Watch for bruising, bleeding, and fall risk due to balance deficits
Pancreatitis
- Description: Inflammation of the pancreas, often due to gallstones or alcohol abuse
- Symptoms: Severe epigastric pain radiating to the back, nausea, vomiting
- PT implications: Monitor for signs of multi-organ failure, avoid activities that increase abdominal pressure
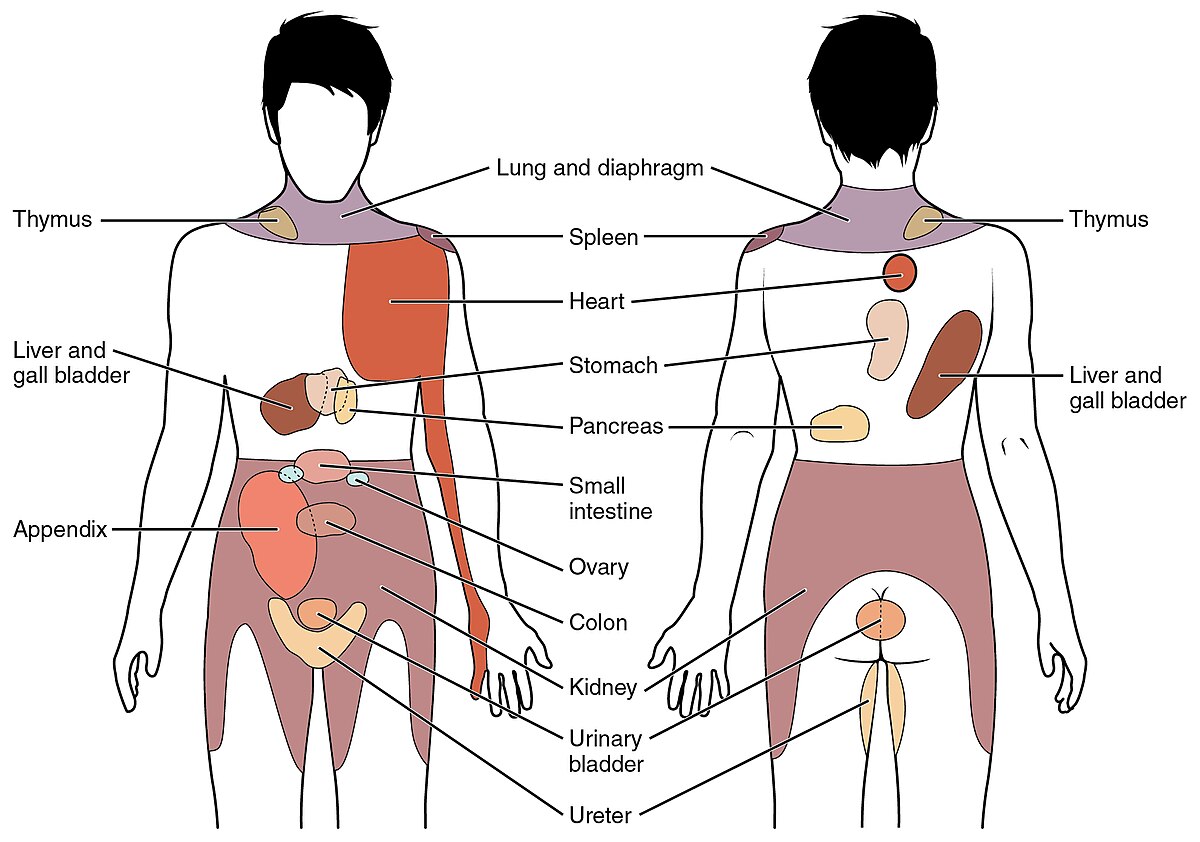
Key referred pain sites
Key clinical patterns:
- Peptic ulcers → Epigastric pain that may radiate to the back
- Pancreatitis → Pain in the mid-back and left shoulder
- Gallbladder issues (Cholecystitis, Gallstones) → Right shoulder, right upper quadrant pain, worsens after fatty meals
- Appendicitis → Periumbilical pain progressing to the right lower quadrant (McBurney’s point)
- Hepatic (liver) issues → Right upper quadrant pain, right shoulder pain, jaundice may be present
- Esophagus → mid chest, mid-back
- Stomach → epigastric region, left upper quadrant, mid-back
- Small intestine → periumbilical region
- Large intestine → lower abdomen, sacral region
- Rectum → sacral region, perineum
Reproductive system
Male reproductive system
Anatomy and physiology
- Primary Structures: Testes, epididymis, vas deferens, seminal vesicles, prostate gland, urethra, and penis
- Function: Produces sperm and male sex hormones (testosterone)
- Hormonal Regulation:
- Hypothalamus → Gonadotropin-releasing hormone (GnRH)
- Pituitary → Luteinizing hormone (LH) & Follicle-stimulating hormone (FSH)
- LH stimulates testosterone production in the testes.
- FSH supports spermatogenesis
Common male reproductive disorders
Benign prostatic hyperplasia (BPH)
- Non-cancerous enlargement of the prostate
- Symptoms: Urinary frequency, nocturia, weak stream, incomplete bladder emptying
- Treatment: Medications (alpha-blockers), surgery if severe
Prostatitis
- Inflammation of the prostate, often bacterial
- Symptoms: Painful urination, pelvic pain, flu-like symptoms
- Treatment: Antibiotics, anti-inflammatories
Prostate cancer
- Most common cancer in men
- Symptoms: Often asymptomatic early, later include urinary dysfunction and bone pain (metastasis)
- Diagnosed with elevated PSA levels, biopsy
- Treatment: Surgery, radiation, hormone therapy
Erectile dysfunction
- Inability to achieve/maintain an erection
- Causes: Vascular disease, diabetes, psychological factors
- Treatment: Medications, lifestyle modifications
Testicular cancer
- Most common in men 15-35 years
- Symptoms: Painless testicular lump, swelling
- Treatment: Surgery (orchiectomy), chemotherapy, radiation
Female reproductive system
Anatomy and physiology
- Primary Structures: Ovaries, fallopian tubes, uterus, cervix, vagina, external genitalia
- Function: Produces eggs, sex hormones (estrogen, progesterone), and supports fetal development during pregnancy
- Hormonal Regulation:
- Hypothalamus → Gonadotropin-releasing hormone (GnRH)
- Pituitary →Luteinizing hormone (LH) & Follicle-stimulating hormone (FSH)
- LH regulates the menstrual cycle, triggers ovulation, and stimulates the ovaries to produce essential steroid hormones like estrogen and progesterone.
- FSH stimulates the ovaries to grow follicles and mature eggs each month.
Common female reproductive disorders
Polycystic ovarian syndrome (PCOS)
-
Hormonal disorder causing irregular ovulation, excess androgens, and ovarian cysts
-
Symptoms: Irregular periods, infertility, insulin resistance, and hirsutism, a condition characterized by excessive hair growth in women in a male-pattern distribution.
-
Treatment: Hormonal therapy, weight management, insulin sensitizers
Endometriosis
- Growth of endometrial tissue outside the uterus
- Symptoms: Pelvic pain, dysmenorrhea, infertility
- Treatment: Pain management, hormonal therapy, surgery
Uterine fibroids
- Non-cancerous tumors of the uterus
- Symptoms: Heavy menstrual bleeding, pelvic pain, infertility
- Treatment: Hormonal therapy, surgery (hysterectomy, myomectomy)
Pelvic inflammatory disease (PID)
- Infection of the female reproductive organs (often due to sexually transmitted diseases)
- Symptoms: Pelvic pain, fever, abnormal vaginal discharge
- Treatment: Antibiotics, hospitalization if severe
Ovarian cancer
- Silent killer due to late detection
- Symptoms: Abdominal bloating, pelvic pain, urinary urgency
- Diagnosis: CA-125 marker, imaging
- Treatment: Surgery, chemotherapy
Breast cancer
- Most common cancer in women
- Risk Factors: Family history, BRCA mutations, hormone exposure
- Symptoms: Lump, nipple changes, skin dimpling
- Treatment: Surgery, chemotherapy, radiation, hormone therapy
Pregnancy considerations for physical therapy
Physiological changes during pregnancy
Musculoskeletal changes
- Increased lumbar lordosis and anterior pelvic tilt →low back pain
- Increased ligamentous laxity due to Relaxin hormone → joint instability, risk of injury
- Widening of the pelvis → sacroiliac (SI) joint pain, pubic symphysis dysfunction
- Diastasis recti (separation of the rectus abdominis)
Cardiovascular changes
- Increased blood volume (40-50%) and heart rate
- Decreased blood pressure in the first and second trimesters (due to vasodilation)
- Risk of supine hypotensive syndrome (compression of the inferior vena cava)
Respiratory changes
- Increased oxygen consumption
- Decreased lung expansion due to elevated diaphragm → shortness of breath
Metabolic changes
- Increased caloric demands.
- Gestational diabetes risk due to insulin resistance.
Other changes
- Increased urinary frequency due to bladder compression
- Weight gain (25-35 lbs is the normal range)
- Hormonal changes (progesterone, estrogen, relaxin) affect mood, joints, and metabolism
- De Quervain’s and carpal tunnel syndrome can both occur during pregnancy due to hormonal changes and fluid retention, which increase pressure on the nerves and tendons in the wrist.
Safe exercise guidelines for pregnancy
- Mode: Walking, swimming, cycling, low-impact aerobics.
- Intensity: Moderate (should be able to talk while exercising)
- Duration: 150 minutes per week (30 min/day, most days)
- Avoid:
- Supine exercises after 20 weeks (risk of supine hypotensive syndrome)
- Overheating (hot yoga, saunas).
- Valsalva maneuver (holding breath during exertion)
- High-impact or contact sports
Contraindications to exercise during pregnancy:
- Absolute:
- Incompetent cervix
- Placenta previa (after 26 weeks)
- Preeclampsia
- Multiple gestation with risk of preterm labor
- Ruptured membranes
- Persistent vaginal bleeding
- Preterm labor
- Relative:
- Severe anemia
- Unevaluated maternal cardiac disease
- Chronic bronchitis
- Poorly controlled diabetes or hypertension
Postpartum considerations
- Pelvic floor dysfunction
- Interventions: Kegels, biofeedback, bladder retraining
- Postural syndromes
- Due to breastfeeding, baby-carrying
- Interventions: strengthening of the upper back, postural correction, stretching
- Return to exercise
- Clearance from physician (typically 6 weeks post-vaginal, 8+ weeks post-C-section)
- Progressive return to impact activities
Incontinence
Types of urinary incontinence and treatment
Stress incontinence
Cause:
- Weak pelvic floor muscles or urethral sphincter dysfunction
- Common in postpartum women, postmenopausal women, and after prostate surgery in men
- Triggered by increased intra-abdominal pressure (e.g., coughing, sneezing, laughing, jumping)
Treatment:
- Pelvic floor muscle training (Kegels) to strengthen muscles
- Bladder training to improve control
- Biofeedback & electrical stimulation for muscle activation
- Pessary (Vaginal) or urethral inserts (in some cases to support and hold pelvic organs in place)
- Surgical options (e.g., sling procedures) for severe cases
Urge incontinence
Cause:
- Detrusor muscle overactivity leads to sudden, strong urges to urinate
- Can be related to neurological conditions (e.g., stroke, Parkinson’s, MS), infections, or idiopathic causes
Treatment:
- Bladder retraining (scheduled voiding, delaying urination)
- Pelvic floor exercises to control urgency
- Behavioral modifications (reducing caffeine, alcohol, and bladder irritants)
- Medications (anticholinergics, beta-3 agonists) to relax the bladder
- Neuromodulation (e.g., tibial nerve stimulation) in severe cases
Overflow incontinence
Cause:
- Incomplete bladder emptying due to obstruction (e.g., enlarged prostate, pelvic organ prolapse) or weak detrusor muscle (e.g., diabetes, spinal cord injury, multiple sclerosis)
- Symptoms include dribbling, a weak stream, and a feeling of incomplete emptying
Treatment:
- Double voiding technique (waiting and trying to urinate again)
- Timed voiding to prevent overflow
- Pelvic floor strengthening is related to muscle dysfunction
- Catheterization (intermittent or long-term) for severe cases
- Surgical intervention if caused by obstruction (e.g., prostate surgery)
Functional incontinence
Cause:
- Physical, structural, or cognitive impairments (e.g., stroke, dementia, arthritis, Parkinson’s, steps to bathroom, physical obstacles) prevent timely access to the bathroom
- No direct bladder dysfunction, but mobility limitations or mental impairments lead to accidents
Treatment:
- Environmental modifications (accessible bathrooms, commodes, grab bars)
- Scheduled toileting based on routine
- Mobility training & assistive devices
- Caregiver education for dementia-related cases
Renal disorders
Common renal disorders
The kidneys play a vital role in filtering waste, regulating electrolytes, and maintaining fluid balance. Dysfunction can lead to serious systemic issues, including metabolic imbalances and cardiovascular complications.
Acute kidney injury (AKI)
Definition: Sudden loss of kidney function due to ischemia, toxins, or trauma. It is often reversible if treated early.
Causes:
- Pre-renal: Hypovolemia, shock, heart failure.
- Intra-renal: Acute tubular necrosis, nephrotoxic drugs, infections
- Post-renal: Obstruction (kidney stones, tumors, BPH)
Signs and symptoms:
- Oliguria (low urine output), fluid retention, electrolyte imbalances (increased potassium, increased BUN/Creatinine)
- Kidney stones (renal calculi) may present with sudden onset of flank pain and blood in the urine, and as the stones travel down the ureter, pain can move to the lower abdomen. Groin and genital region,
PT considerations:
- Monitor for fatigue, altered mental status, and electrolyte imbalances
- Avoid overexertion due to risk of hypotension and electrolyte shifts
Chronic kidney disease (CKD)
Definition: Progressive decline in kidney function, leading to end-stage renal disease (ESRD) if untreated
Causes:
- Diabetes (leading cause), hypertension, glomerulonephritis, polycystic kidney disease
Stages (GFR-based):
- Stage 1-2: Mild kidney damage, no major symptoms.
- Stage 3: Moderate impairment, possible anemia, bone mineral disorders
- Stage 4: Severe dysfunction, preparing for dialysis
- Stage 5 (End Stage Renal Disease): Requires dialysis or a kidney transplant
Signs and symptoms:
- Fatigue, muscle cramps, edema, anemia, metabolic acidosis, hypertension, itching
- Uremia (buildup of waste in blood) → nausea, confusion, neuropathy
- Pruritus is a very itchy skin that is most common in patients with advanced CKD and end-stage kidney disease (ESRD)
PT considerations:
- Monitor for fatigue, blood pressure changes, and electrolyte imbalances
- Encourage low-to-moderate intensity exercise to improve functional capacity
- Avoid excessive fluid loss (dehydration can worsen kidney function)
- Be aware of bone mineral disease & risk of fractures
Nephrotic syndrome
Definition: A kidney disorder causing severe protein loss in urine due to damage to the glomeruli
Signs and symptoms:
- Severe edema (especially in the legs), proteinuria (>3.5g/day), hypoalbuminemia, hyperlipidemia.
- Increased risk of thrombosis and infections
PT considerations:
- Monitor for edema-related mobility restrictions
- Be cautious of increased clotting risk during exercise
Hemodialysis (HD) considerations
Hemodialysis is used in ESRD to filter blood through a machine when the kidneys can no longer perform their function. It is typically done 3-4 times per week for 3-5 hours per session.
Common complications:
- Hypotension during or after dialysis (due to rapid fluid removal)
- Fatigue, dizziness, cramping (electrolyte shifts)
- Access site issues (fistula/graft infections, thrombosis)
PT considerations:
- Avoid exercise immediately before or after dialysis due to fatigue and hypotension risk
- Monitor blood pressure carefully – hypotension is common post-dialysis
- Exercise should be performed on non-dialysis days or at least 4+ hours after treatment
- Do not take blood pressure on the arm with an AV fistula/graft to prevent complications
- Encourage low-impact aerobic and resistance exercises to improve endurance and prevent muscle wasting