Excretory and reproductive systems
Excretory system
The excretory system helps maintain homeostasis in several key ways. It regulates blood pressure, osmoregulation, ion balance, acid-base balance, and removes nitrogenous waste:
-
Blood pressure:
If blood pressure is too low, the kidney’s juxtaglomerular apparatus releases renin, which starts the renin-angiotensin pathway and ultimately produces angiotensin II.
Angiotensin II stimulates the adrenal glands to secrete aldosterone, which prompts the kidney distal tubules to reabsorb more Na⁺ (and therefore more water). At the same time, ADH from the hypothalamus/pituitary can further increase water reabsorption. High levels of ADH also promote vasoconstriction, and both effects raise blood pressure.
Conversely, if blood pressure is too high, production of these hormones decreases. The heart also secretes ANP (atrial natriuretic peptide), which antagonizes aldosterone so the kidneys excrete more Na⁺ and water, and it can also promote vasodilation. -
Osmoregulation:
Blood osmolarity depends mainly on and . When osmolarity is low, aldosterone promotes reabsorption of , with often following. The kidney tubules adjust fluid composition by selectively secreting and reabsorbing ions, which helps keep osmotic balance stable. -
Ion balance:
excretion is regulated by aldosterone (as is reabsorbed, is lost). Meanwhile, PTH (parathyroid hormone) regulates calcium and phosphate levels by increasing reabsorption in the kidney and mobilizing it from bone. -
Acid-base balance:
The body’s primary buffer system uses bicarbonate (). Exhaling via respiration reduces acidity, while the kidney tubules can excrete or reabsorb bicarbonate ion and secrete as needed to stabilize blood pH. -
Nitrogenous waste:
The kidneys eliminate soluble waste, especially urea, a less toxic product of ammonia metabolism. This waste, along with water and salt, forms urine, which is excreted to keep the internal chemical environment stable.
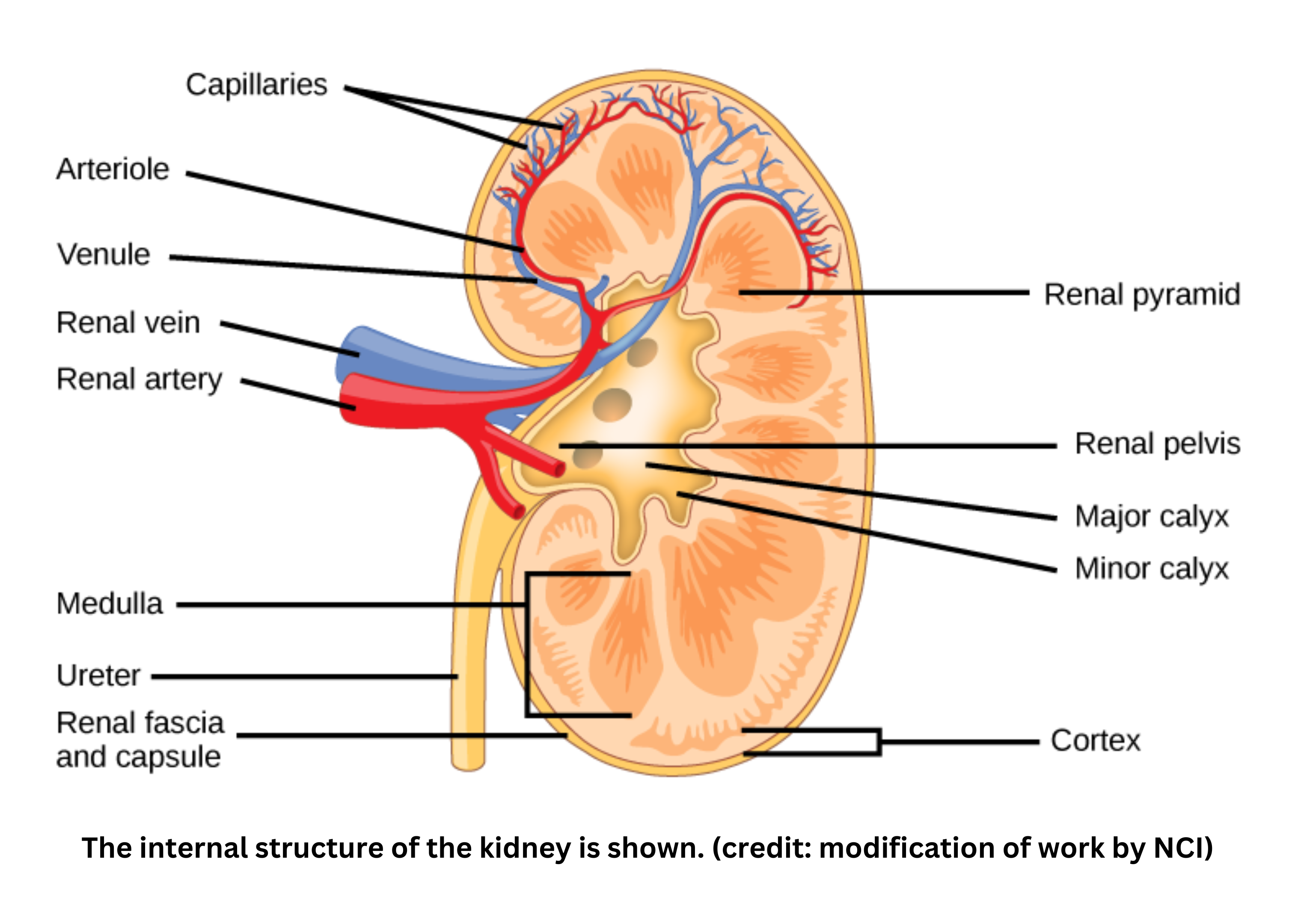
Kidney structure
- The kidney has an outer region called the cortex, where most convoluted tubules are found, and an inner region called the medulla, which contains the loop of Henle. The kidney’s functional unit is the nephron, which includes the glomerulus, Bowman’s capsule, the proximal tubule, the loop of Henle, the distal tubule, and the collecting duct.
Nephrons
- In each nephron, the glomerulus is a ball of fenestrated capillaries where filtration begins. It’s surrounded by Bowman’s capsule, a cup-like structure that collects the filtrate.
- The proximal tubule is the main site of nutrient and salt reabsorption, and it also carries out secretion of various substances (except potassium, which is mainly handled by the distal tubule under aldosterone regulation).
From the proximal tubule, filtrate flows into the loop of Henle, a U-shaped loop that dips into the renal medulla and carries out the countercurrent multiplier mechanism. The descending limb is permeable to water but not solutes, so water leaves by osmosis and the filtrate becomes more concentrated near the bottom of the loop.
The ascending limb is impermeable to water but allows salt to diffuse or be actively transported out, which dilutes the filtrate as it moves upward. - The filtrate then enters the distal tubule, which fine-tunes electrolyte and water reabsorption (and secretes potassium under aldosterone influence). Multiple distal tubules drain into a shared collecting duct, where ADH controls water permeability and additional hormone-regulated salt transport helps finalize urine composition.
Formation of urine
- Glomerular filtration uses hydrostatic pressure to push fluid and small solutes (including nutrients and waste products) from the blood into Bowman’s capsule. Both “good” substances (like glucose and amino acids) and “bad” substances (like urea, creatinine, and uric acid) enter the filtrate. As the filtrate moves through the proximal tubule, valuable nutrients and most ions are selectively reabsorbed back into the bloodstream, while waste products are secreted for eventual excretion.
- The filtrate then enters the loop of Henle, which uses the countercurrent multiplier mechanism to create an osmotic gradient in the renal medulla. Its descending limb is permeable to water but not solutes, so water exits by osmosis; by the bottom of the loop, the filtrate becomes highly concentrated.
- The ascending limb, in contrast, is impermeable to water but actively transports salts out, driven by a pump, which dilutes the filtrate.
- In the distal tubule, hormone regulation (especially aldosterone) fine-tunes ion and fluid balance by reabsorbing sodium and secreting excess potassium.
- Final adjustments occur in the collecting duct, where ADH (antidiuretic hormone) controls water reabsorption into capillaries based on the osmotic gradient - largely established by salt pumping and urea recycling - which concentrates the urine when needed.
- At the same time, the kidneys help maintain blood pH by secreting when blood is too acidic or excreting bicarbonate when blood is too alkaline. The overall process produces urine rich in nitrogenous waste, mainly ammonia converted to the safer compound urea.
- Urine drains from nephrons into the ureter, which carries it to the bladder - a muscular reservoir lined with transitional epithelium that can stretch as it fills. When the bladder is sufficiently full, urine exits through the urethra, completing the excretory pathway. Sphincter muscles control release by contracting to retain urine and relaxing to allow expulsion.
Reproductive system
Male and female reproductive structures and their functions
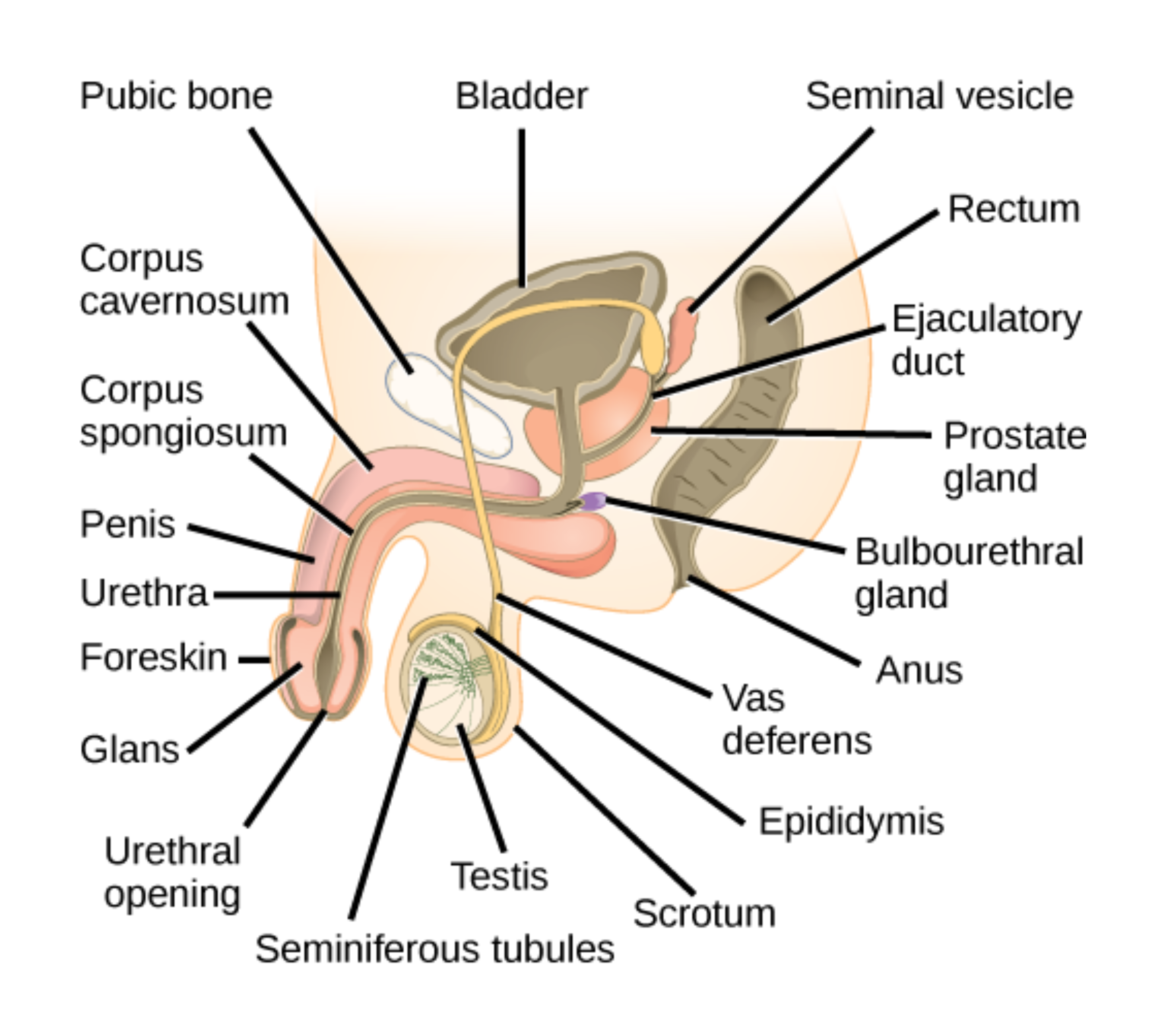
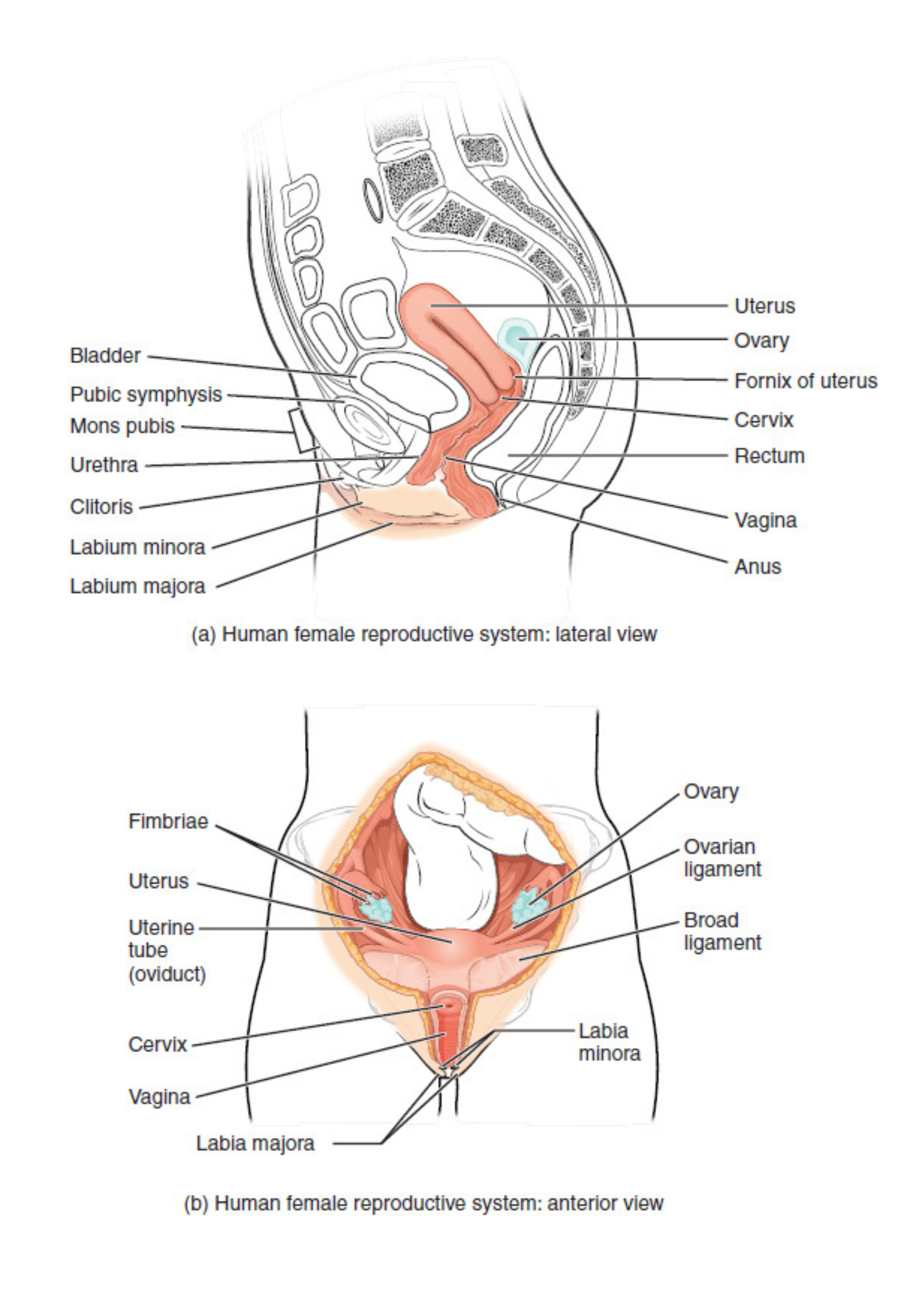
- The gonads are the primary reproductive organs. In males, the testes produce sperm in the seminiferous tubules and secrete testosterone. In females, the ovaries contain immature oocytes and produce estrogen. Male reproductive structures are largely external, while female structures are primarily internal.
In males, sperm move from the seminiferous tubules to the epididymis for storage, then travel through the vas deferens and ejaculatory duct into the urethra, exiting through the penis.
In females, an oocyte matures each month inside a follicle in the ovary. The fallopian tubes receive the released egg, and fertilization may occur as it travels toward the uterus. In the uterus, a thickened endometrium either supports embryo implantation or is shed during menses (if fertilization does not occur). The vagina is the canal connecting the uterus to the external environment.
Hormonal control of reproduction
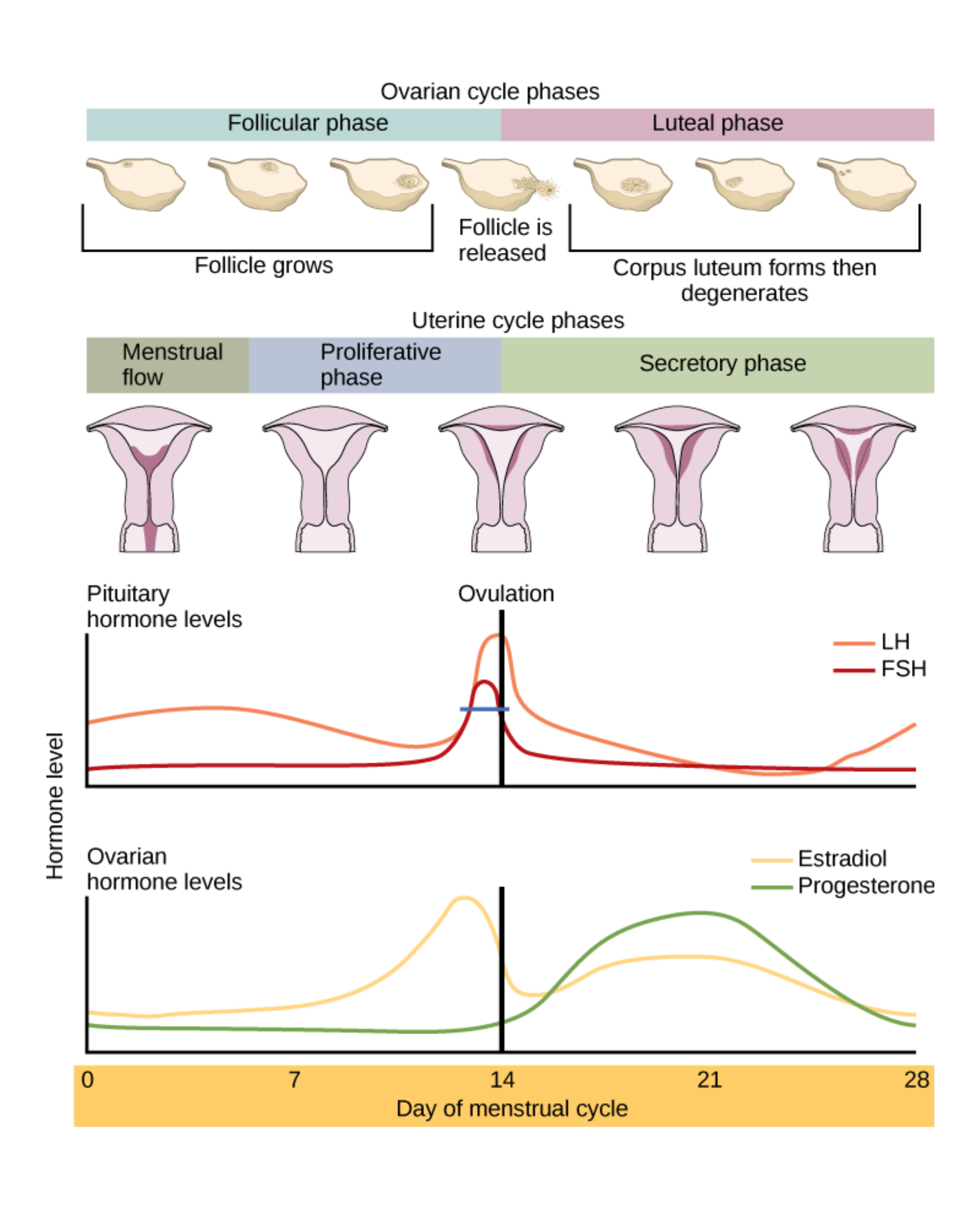
- Control of the female cycle begins with GnRH from the hypothalamus, which triggers release of FSH (follicle-stimulating hormone) and LH (luteinizing hormone).
FSH promotes follicle growth and estrogen production. Estrogen usually inhibits FSH and LH until it reaches a threshold; at that point, it triggers an LH surge, which causes the follicle to rupture and the primary oocyte to become a secondary oocyte. The ruptured follicle becomes the corpus luteum, which releases estrogen and progesterone to maintain the endometrium.
If fertilization does not occur, the corpus luteum atrophies, hormone levels fall, and menstruation begins. If fertilization occurs, the embryo secretes hCG, which mimics LH and preserves the corpus luteum until the placenta can take over hormone production.
Male hormonal control of reproduction begins at puberty. The hypothalamus releases GnRH, which prompts the anterior pituitary to secrete FSH and LH. FSH stimulates Sertoli cells in the testes to support spermatogenesis, while LH stimulates Leydig cells to produce testosterone. Testosterone drives secondary sexual characteristics (such as a deepened voice, increased body hair, and sex drive) and also supports spermatogenesis.
This system is regulated by negative feedback: high testosterone levels signal the hypothalamus and anterior pituitary to reduce release of GnRH, FSH, and LH, which moderates sperm production. Sertoli cells also secrete inhibin when sperm count is high, further suppressing these hormones. When sperm count is lower, less inhibin is secreted, allowing hormone levels to rise and stimulate more spermatogenesis.
Comparing the sexes, the male reproductive tract merges with the urinary tract and is largely external, supporting spermatogenesis in the testes and frequent opportunities for fertilization. The female tract is mostly internal and separate from the urinary system. Oogenesis in the ovaries occurs cyclically, creating a monthly opportunity for fertilization.
Pregnancy, parturition, lactation
- Hormonal changes during pregnancy
- During pregnancy, hCG maintains the corpus luteum, which secretes progesterone until the placenta takes over that role. As pregnancy progresses, estrogen levels rise along with progesterone. Near childbirth, the balance shifts: progesterone drops to allow uterine contractions, while estrogen supports growth of the myometrium and increases oxytocin receptor expression to support labor.
- Parturition
- Parturition means childbirth. During gestation, high progesterone suppresses uterine contractions. As progesterone levels fall before birth, the uterus can contract more strongly, and estrogen-driven increases in oxytocin receptors make the uterus more responsive. Rising oxytocin then strengthens uterine contractions. Cervical dilation and uterine distention further increase oxytocin release in a positive feedback loop, leading to delivery.
- Lactation
- After birth, progesterone and estrogen levels drop sharply, which removes their inhibition of the milk duct system (the lactiferous ducts). Prolactin remains elevated and promotes milk production (galactopoiesis).
- Oxytocin triggers contraction of smooth muscle around alveoli, producing the “milk letdown” reflex when the nipples are stimulated. Prolactin is required for milk production, while oxytocin is required for milk secretion.