
Acquired disorders
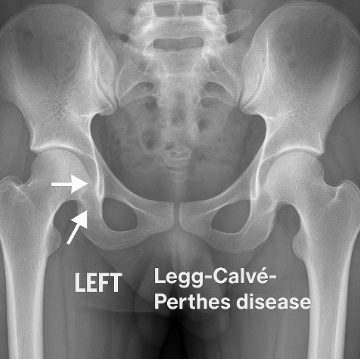
Legg-Calve Perthes disease
Phases of Legg-Calve Perthes:
- 1.) Necrosis-part of the femoral head has died,
- 2.) Fragmentation- the body attempts to clean up the broken pieces of bone from the area
- 3.) Re-ossification- blood flow is restored to the femoral head, and the bone begins to re-grow,
- 4.) Remodeling- new bone is new in place.
Symptoms include:
- Antalgic gait
- Pain/stiffness in thigh/groin
- Leg length discrepancy
- Limitations in range of motion- abduction, flexion, and internal rotation
Physical therapy interventions and Legg-Calve Perthes disease
- Activity modifications
- Bracing/splinting to keep the femoral head in contact acetabulum
- Strengthening and range of motion activities of the hip
Medical management of Legg-Calve-Perthes disease
- Use of anti-inflammatory medications
- Surgical interventions to correct blood flow- not indicated for children under 6
Slipped-capital epiphysis
Symptoms
- Inability to bear weight on the extremity
- Pain in the groin/thigh
- Leg length discrepancy
- Limitations in range of motion- flexion, internal rotation, and abduction
Medical management and slipped-capital epiphysis
Surgery is indicated once confirmed through physical examination and X-ray imaging. Delay in intervention can cause serious damage such as avascular necrosis, arthritis, or deformity of the hip joint. Surgery entails the implementation of a metal screw to maintain the position of the femoral neck through the growth plate.
Physical therapy intervention and slipped-capital epiphysis
Physical therapy interventions are dependent upon the surgeon’s protocol post-op and will gauge the progression of activities until return to full weight bearing.
Osgood-schlatter
Symptoms
- Palpable swelling at the tibial tuberosity
- Pain at anterior knee
- Increased pain during running, jumping activities , with relief of pain during rest
Physical therapy interventions and Osgood-Schlatter
- Strengthening of lower extremity muscles to create an even pull of muscles
- Dynamic balance activities to mimic times of exacerbation
- Postural re-education when performing running, jumping activities
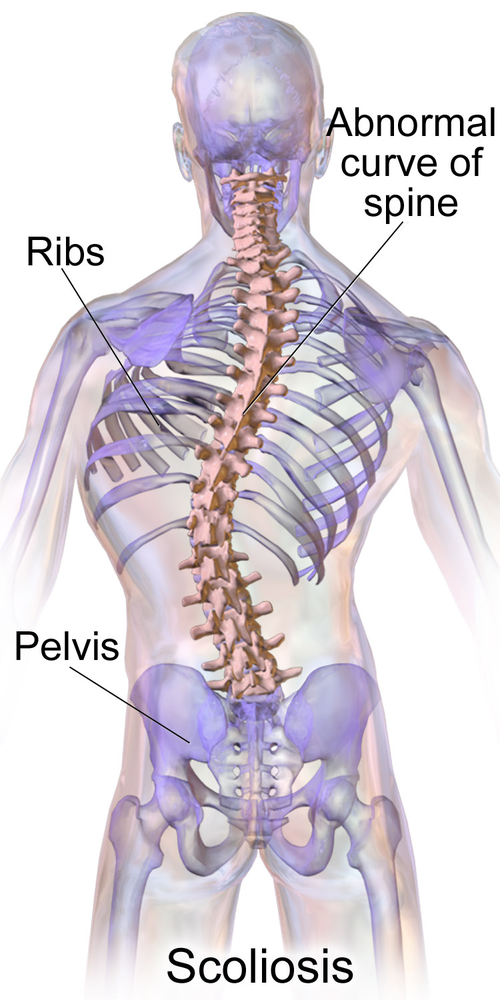
Scoliosis
Cobb angle (severity of scoliosis):
- Mild scoliosis: Cobb angle less than 10 degrees
- No intervention or conservative management
- Moderate scoliosis: Cobb angle between 10 and 25 degrees
- Bracing and physical therapy may be indicated
- Severe scoliosis: Cobb angle greater than 25 degrees
- Surgical intervention to correct the curve , as a curve >25 degrees could compromise the respiratory system
Symptoms
- Uneven shoulders
- One shoulder blade that appears more prominent than the other
- Uneven waist
- One hip is higher than the other
- One side of the rib cage jutting forward
Physical therapy interventions and scoliosis
- Address muscle imbalances that may be present due to curvature
- Provide shoe inserts to correct leg length discrepancy
- Prescribe durable medical equipment as necessary
Autism spectrum disorder
Symptoms
- Sensory integration dysfunction
- Hyposensitive (sensory seeking) or hypersensitivity (sensory avoidant)
- Difficulty with verbal and non-verbal communication
- Impaired coordination
- Balance deficits
- Occasional strength and range of motion deficits
- Developmental delay
Physical therapy and autism spectrum disorder
- Address developmental delay
- Improve strength
- Improve balance and coordination
- Sensory integration activities
- Be aware that new people and situations can cause either withdrawal behavior or increased aggression
Brachial plexus injuries
Severity of brachial plexus injuries is as follows:
- Traction
- Stretching of the nerve with spontaneous recovery
- Rupture
- Nerve is torn but remains attached to the spinal cord; may require surgical intervention
- Avulsion
- Nerve is completely torn from the spinal cord; permanent disability may result after surgical intervention
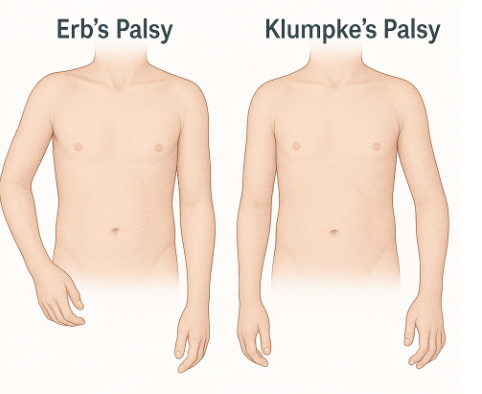
Common brachial plexus injuries
- Erb’s palsy
- Involves C5-C6 nerve roots- upper arm paralysis involving rhomboids, serratus anterior, levator scapula, deltoid, infraspinatus, supraspinatus, biceps
- Immobility of the shoulder girdle leading to subluxation of the shoulder
- Only use of hand muscles
- Involves C5-C6 nerve roots- upper arm paralysis involving rhomboids, serratus anterior, levator scapula, deltoid, infraspinatus, supraspinatus, biceps
- Klumpke’s palsy
- Involve s C8-T1 nerve roots- lower arm paralysis involving intrinsic muscles of the hand, finger flexors, and finger extensors
- Contractures of the hand may result
- Functional use of the shoulder and elbow; deficits in the use of the wrist and hand
- Involve s C8-T1 nerve roots- lower arm paralysis involving intrinsic muscles of the hand, finger flexors, and finger extensors
- Global palsy
- Involves C5-T1- total arm paralysis
Physical therapy interventions and brachial plexus injuries
- Partial immobilization for 1-2 weeks of the injured extremity
- Constraint-induced therapy of the non-injured arm
- Range of motion to avoid contractures
- Age-appropriate movements to decrease the likelihood of developmental delay
- Parent education on positioning and handling of the infant
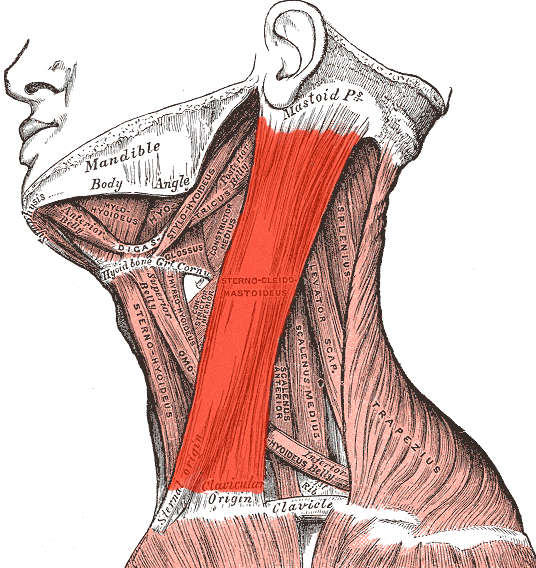
Tortocolis
Symptoms:
- Persistent head tilt to one side
- Difficulty turning the head to the opposite side
- A lump or knot may be felt in the tight neck muscle
- Facial asymmetry may develop over time
- Flat head on the side of muscle tightness may present (plagiocephaly)
Physical therapy interventions and torticollis
- Stretching of the contracted sternocleidomastoid muscle
- Positioning to allow for prolonged stretched
- Addressing any developmental delay issues