



Congenital disorders
Cerebral palsy
Types of cerebral palsy
- Spastic cerebral palsy (Hypertonic cerebral palsy)
- Type of cerebral palsy in which the individual exhibits hypertonia, causing stiff and jerky movements
- Spastic hemiplegia
- Hypertonia is located on one side of the body; the ipsilateral arm and leg
- Side of dysfunctions is typically shorter and thinner, scoliosis may be present, and intellect is normal
- Spastic diplegia
- Hypertonia is located primarily in the lower extremities
- Hyperreflexia can be present, scissoring of gait, and intellect is normal
- Spastic quadriplegia
- Hypertonia is located throughout the entire body
- The most severe type of spastic cerebral palsy is due to widespread damage to the entire brain
- Individuals with this type of CP rarely walk, demonstrate difficulty speaking, and can have some intellectual difficulty
- Spastic hemiplegia
- Type of cerebral palsy in which the individual exhibits hypertonia, causing stiff and jerky movements
- Hypotonic cerebral palsy
- Characterized by low tone and floppiness of extremities and axial skeleton
- Individuals may demonstrate poor muscle tone, excessive range of motion, increased weight gain, impaired speech due to poor oral motor control, and wide base support with gait
- Dyskinetic cerebral palsy (Athetoid cerebral palsy)
- Characterized by slow and uncontrollable writhing or jerky movements of the hands, feet, arms, and legs
- Individuals may demonstrate postural deficits, hearing problems, and breathing difficulties; their intellect remains intact
- Ataxic cerebral palsy
- Characterized by poor coordination, balance impairments, and impairments in depth perception
- Individuals may demonstrate a wide base of support, dysmetria, and difficulty with the precision of movements
- Mixed types
- Characterized by mixed muscles of hypertonia and hypotonia with varied symptom presentation
Classifications of cerebral palsy
-
Level I: Walks without limitations (mild).
-
Level II: Walks with some limitations, needs aids for long distances.
-
Level III: Walks with assistive devices (walkers, crutches).
-
Level IV: Limited mobility, mostly uses wheelchairs.
-
Level V: Severe mobility impairment, needs power wheelchair and significant assistance (severe).
Physical therapy interventions for cerebral palsy
- Positioning is key to promote improvements in mobility, ADL participation, gait and balance improvements, and interaction with the environment.
- Symmetrical posture
- Alignment of trunk, pelvis, and extremities
- Head in midline
- Hips and knees in 90 degrees in sitting
- Prescription of orthoses
- Optimizing functional motor skills
- Treatment of visual-motor and perceptual disorders
- Aids to assist with visual processing, aiding in connecting the visual system to the brain
- Treatment of orthopedic conditions such as
- Scoliosis
- Joint contractures
- Kyphosis
- Clubfoot
- Hip or shoulder dislocation
Medical management for cerebral palsy
- Anti-seizure medication
- Spasticity mediation
- Botox injections for local hypertonic muscles
- Baclofen taken orally or by implantation for multiple areas of hypertonia
- Surgical interventions
- Dorsal rhizotomy:
- Dorsal nerve roots are served to aid in decreasing spasticity and improving overall function
- Z-plasty
- Release of muscle or tendons to release contractures
- Dorsal rhizotomy:
Down syndrome
Characteristics of Down syndrome include:
- Small ears and a protruding tongue
- Microcephaly with flattened occiput
- Short stature
- Hypotonia and hypermobility
- Congenital heart defects
- Speech deficits
- Developmental delays
- Vertebral instability at the atlanto-axial joint (C1-C2)
- Intellectual disabilities
Physical therapy interventions for Down syndrome
- Promote gross motor development
- Increase motor control and postural awareness
- Improve oral-motor development
- Durable medical equipment recommendations as appropriate
- Patient and family education
Special considerations with Down’s syndrome
- Avoidance of diving, tumbling, headstands, and contact sports due to increased risk for hyperflexion injuries due to atlanto-axial instability
Duchenne muscular dystrophy
Common symptoms of Duchenne muscular dystrophy
- Progressive muscle weakness
- Pseudohypertrophic muscles appear hypertrophied, but the muscle has been replaced by fat and connective tissue in calves, deltoids, quadriceps, and tongue
- Contracture
- Cardiac myopathy
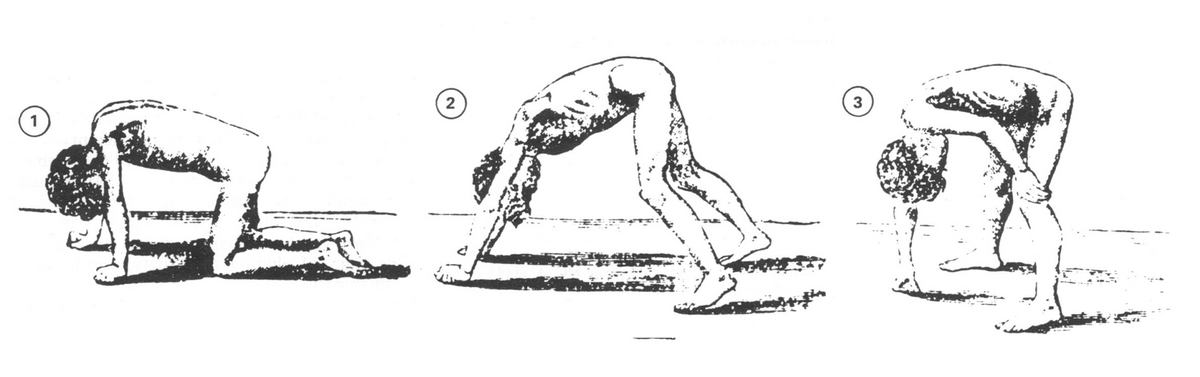
- Gower’s sign
- The child pushes up from the floor with their hands, walking their hands up their legs to stand- this is due to weak hip and knee extensors; typically begins at ages 4-7
- Waddling gait
- Increased risk of falls
Progression of Duchenne muscular dystrophy
- Age 3-5: weakness, tripping, Gower’s sign is present
- Age 9-11: gait deviations leading to high energy expenditure occur, unable to ascend/ descend stairs; poor endurance; bracing may be required for ambulation; loss of ability to ambulate occurs
- Age 12-14: use of manual wheelchair, increased weight gain, contracture of lower extremity joints
- Age 15-17: increased respiratory compromise, total dependence for ADL, and all mobility
- Young adulthood: death in early 20s due to respiratory compromise
Physical therapy interventions for Duchenne muscular dystrophy
- Maintain range of motion
- Assess mobility and attempt to maintain the current level of mobility
- Provide durable medical equipment as appropriate
- Parent and patient education
Medical management for Duchenne muscular dystrophy
- Treatments of symptoms as appropriate
- Use of medications such as steroids, antibiotics as needed
- Treatment of orthopedic conditions through injections or surgery
Spinal muscular atrophy (SMA)
Five types of SMA:
- Type 0 (Zero)
- Presents at birth; muscle atrophy and severe muscle weakness present; leads to life-threatening respiratory compromise
- Type 1 (Infantile)
- Presentation within the first 6 months of life; muscle weakness specifically impacting feeding, crawling, and sitting
- Type 2 (intermediate)
- Presentation between 6-18 months of life; progressive muscle weakness in the hips, legs, and trunk
- Type 3 (Juvenile)
- Presentation between 18 months and -18 years; muscle weakness in the back, legs, and feet
- Type 4 (Adult)
- Presentation after 18 years of age; mild symptoms that present later in life
Physical therapy interventions for SMA
Physical therapy interventions are based upon the level of impairment associated with the SMA and can include progression to meet developmental milestones, improvements in range of motion, improvements in balance, improvements in posture, strengthening muscles, and initiation of energy conservation strategies.
Spina bifida
Common symptoms associated with spina bifida are:
- Flaccid or spastic paralysis
- Bladder incontinence
- Musculoskeletal deformities (scoliosis, hip dysplasia, hip dislocation, club foot, hip/knee contracture)
- Hydrocephalus, along with Type I or II Arnold-Chiari malformation
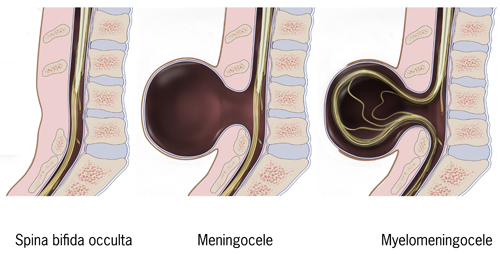
Three (3) types of spina bifida:
- Spina bifida occulta
- No spinal cord involvement
- Depression or dimple in the lower back
- A small patch of dark hair
- Soft fatty deposits
- Port-wine nevi (deep red-purple macular lesions)
- Minimal disability, if any
- Spina bifida meningocele
- No spinal cord involvement
- Meninges protrude through the skin
- Cerebrospinal fluid may leak
- Associated diagnoses: club foot, hip dysplasia, hydrocephalus
- Moderate disability
- Spina bidia myelmeningocele
- Spinal cord involvement
- Protrudes through the skin
- Severe disability will result
- Paralysis usually occurs
Physical therapy and spina bifida interventions
- Joint ROM
- Axial and trunk strengthening and engagement
- Positioning and handling (specifically for infants)
- Mobility and balance
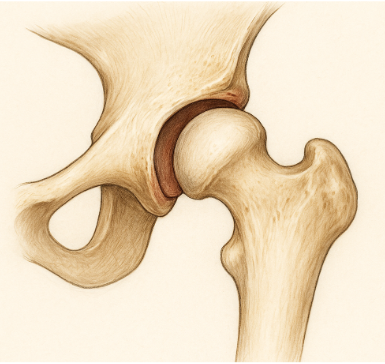
Developmental dysplasia of the hip (DDH)
Common symptoms are:
- Leg length discrepancy (affected leg is shorter than the unaffected)
- Increased folds in the skin of the thigh/buttocks of the affected extremity
- Increased popping noted when moving the affected leg
- Ortalani test
- Movement in flexion and abduction to 90 degrees causes an audible clunk or pop when attempting to perform
- Barlow test
- Movement in flexion and adduction to 90 degrees causes an audible clunk or pop when attempting to perform
- Ortalani test
Physical therapy interventions and DDH
- Education provided to the family for the appropriate positioning of the infant to reduce hip dislocation occurrence
- Gentle range of motion activities that do cause dislocation
- Wearing of Pavlick harness
- The Pavlick harness is a soft splint used to allow for consistent contact between the acetabulum and the femoral head
- Positioned in abduction of legs, hip flexion, and knee flexion through a series of straps to keep the infant in this position
- Used for infants 6 months or younger with the goal of 24-hour wearing for the first 6 weeks and progressing to 6 weeks of wearing only at night
- The parents must learn how to care for the baby fully during the time of consistent wearing
- Change from wearing 24 hours a day to only a night is determined by an orthopedic physician via x-ray and ultrasound
- Developmental delay may occur in an infant due to constant positioning, as mentioned above, with decreased ability to move out of position
- The Pavlick harness is a soft splint used to allow for consistent contact between the acetabulum and the femoral head
Club foot
Phases of intervention are as follows:
- Phase 1: serial casting
- Club foot is stretched/manipulated to improve the range of motion, and then a hard cast is set in place over the affected extremity
- The hard cast is removed, and stretching occurs again, with a new cast put in place with the new range of motion that has been achieved
- The goal is to wear the hard cast until normal alignment is achieved - can take 4-10 weeks to achieve normal alignment
- Club foot is stretched/manipulated to improve the range of motion, and then a hard cast is set in place over the affected extremity
- Phase 2: bracing
- Once serial casting is complete (normal alignment is achieved), bracing is put in place to aid in maintaining the normal alignment of the foot
- The timeframe for bracing can vary depending on the severity of the original club foot deformity
- Once serial casting is complete (normal alignment is achieved), bracing is put in place to aid in maintaining the normal alignment of the foot
Physical therapy interventions
Physical therapy is important in performing serial casting, recommending appropriate bracing options, and intervening if any developmental delays have occurred due to club foot and/or club foot interventions.
Osteogenesis imperfecta
Symptoms of osteogenesis imperfecta:
- Short stature
- Joint laxity,
- Frequent fractures
- Bone deformities,
- Muscle weakness,
- Hearing loss
- Dental problems.
Physical therapy interventions and osteogenesis imperfecta
Education is provided to parents on swaddling techniques, positioning, handling, and fall prevention techniques as progression through developmental milestones.
Arthrogryposis multiplex congenita (AMC)
Clinical presentation
- Multiple joint contractures at birth (e.g., clubfoot, extended knees, flexed wrists)
- Muscle hypoplasia or replacement of muscle tissue with fibrous or fatty tissue
- Thin, atrophic limbs
- No progressive neurological decline
- Normal cognitive function in most cases
Common postural patterns:
- Shoulders: Internal rotation and adduction
- Elbows: Extended or flexed, depending on the subtype
- Wrists: Flexed and ulnarly deviated
- Hands: Clenched with thumb-in-palm deformity
- Hips: Abducted and externally rotated or dislocated
- Knees: Hyperextended or flexed
- Feet: Clubfoot (equinovarus) deformities
Medical and physical therapy management
Physical therapy interventions
- Passive range of motion (PROM): Initiated early to maintain or improve joint flexibility
- Stretching: Daily stretching programs to prevent worsening
- Positioning: Using splints or orthoses to maintain joint alignment
- Serial casting: For correcting severe deformities gradually
- Strengthening exercises: Focused on available muscle groups
- Mobility training: Use of assistive devices (walkers, wheelchairs, KAFOs)
- Gait training (if lower extremities involved)
Orthotic management
- AFOs or KAFOs for ambulation
- Hand splints to improve function
- Spinal orthoses if scoliosis develops
Surgical interventions
- Tendon transfers
- Joint release
- Clubfoot correction (e.g., Ponseti method or surgical release)
- Hip or knee reconstructions in severe deformities