Cardiac exercise testing
Types of test
- 6-minute walk test
- Test goal: measure distance walked in 6 minutes with or without an assistive device
- Rationale: test for endurance related to cardiovascular health
- Setting used: Phase I and Phase II of cardiac rehabilitation
- Test advantages: Quick assessment of endurance that can be completed for lower-level patients
- Graded exercise testing
- Test goal: assess the maximal workload that can be applied to the cardiovascular system via treadmill testing at different grades (incline)
- Rationale: provide the therapist with information on the highest capacity of exercise tolerance
- Provides the maximal heart rate that can be used to then give the target heart range with activity
- Setting: Phase II cardiac rehabilitation
- Test advantages: Most accurate assessment tool of an individual’s exercise tolerance
- Cycle ergometer test:
- Test goal: A submaximal graded exercise test used to estimate VO₂ max and assess cardiovascular endurance by progressively increasing cycling resistance/workload.
- Rationale: provides the maximum amount of oxygen your body can use during intense exercise, serving as the best indicator of your cardiovascular fitness and aerobic endurance.
- Setting: Phase II cardiac rehabilitation
- Test advantage: Utilized over maximal exercise testing if the patient is unable to tolerate maximal testing parameters
Contraindications for exercise testing
- Unstable angina
- Acute myocardial infarction
- Acute congestive heart failure
- Uncontrolled arrhythmias
- Systolic blood pressure >200 mmHg or diastolic blood pressure >115 mmHg
- Severe anemia
- Hemoglobin less than 8
- Advanced or complicated pregnancy
Reasons to stop exercise testing
- Severe ST-segment depression of 2mm or greater
- Cardiac arrest
- Development of new 2nd or 3rd degree heart block
- Patient requests to stop
- Severe chest pain, dizziness, or dyspnea
- Fall in systolic blood pressure <20 mmHg
- Ataxia
- Rise in systolic blood pressure >200 mmHg or diastolic > 110 mm Hg
Cardiac medications
- Beta blockers (atenolol): hypertension medication
- Mechanism of action: works on the heart muscle by blocking epinephrine; decreased heart rate
- PT implications: do not use heart rate as an indicator for response to exercise; use the perceived exertion scale (RPE) to assist with tolerance to activity
- Calcium channel blockers: hypertension medication
- Mechanism of action: works on the heart muscle to prevent calcium from entering heart tissue; increases vasodilation; decreases heart rate
- PT implications: orthostatic hypotension
- Angiotensin converting enzyme inhibitors (ACE Inhibitors): hypertension medications
- Mechanism of action: works on the kidneys to stop the conversion of Angiotensin I to converting to Angiotensin II and causes vasodilation in the peripheral vascular system
- PT implications: Orthostatic hypotension, dizziness, palpitations
- Diuretics (lasix & hydrochlorothiazide): hypertension medication
- Mechanism of action: works on the kidneys to decrease the fluid retention in the body by moving sodium out of the body
- PT implications: electrolyte imbalance, orthostatic hypotension, muscle cramps, increased urination
- Anticoagulants (warfarin, coumadin): decreases clotting of blood
- Mechanism of action: works to reduce the clotting within the blood
- PT implications: hemorrhage risk, can easily bruise
- Nitroglycerin: used specifically for angina pectoris
- Mechanism of action: works to relax smooth muscle in the heart, releasing nitric oxide, which will cause vasodilation and a reduction in blood pressure
- Specifically used in angina pectoris
- PT implications: dizziness, headache, weakness, nausea
- Mechanism of action: works to relax smooth muscle in the heart, releasing nitric oxide, which will cause vasodilation and a reduction in blood pressure
- Digitalis (digoxin): Medication commonly used to treat heart failure and certain atrial dysrhythmias.
- Mechanism of action: Increases the force of myocardial contraction (positive inotropic effect) and slows conduction through the AV node, which helps decrease heart rate.
- PT implications: Monitor heart rate, rhythm, blood pressure, and signs of digoxin toxicity. Patients with renal impairment are at increased risk for digoxin toxicity because digoxin is primarily excreted by the kidneys. Toxicity may lead to nausea, vomiting, visual disturbances, dysrhythmias, dizziness, and possible hospitalization.
- Antihyperlipidemias (statins): cholesterol medication
- Mechanism of action: blocks the production of cholesterol by the liver
- PT implications: muscle pain, muscle weakness, fatigue, diarrhea, constipation, headache
- Amiodarone (antiarrhythmic agent): unstable ventricular tachycardia and recurrent ventricular fibrillation medication
- Mechanism of action: increases the duration of the action potential as well as the effective refractory period for cardiac cells
- PT implications: signs of congestive heart failure, including dyspnea, rales/crackles, peripheral edema, jugular venous distention, and exercise intolerance
Observational cardiac topics
Pulse (also known as heartbeat or rhythm)
- 0: Absent – No pulse is palpable, even with maximum pressure. (Requires immediate medical evaluation).
- 1+: Thready or Weak – Barely perceptible; it fades in and out and can be easily obliterated with slight pressure.
- 2+: Diminished – Easily palpable but weaker than a normal, expected pulse.
- 3+: Normal – Easily felt, full, and requires moderate pressure to obliterate.
- 4+: Bounding – Very strong and hyperactive; it does not disappear even with moderate to firm pressure
Pitting edema grading (associated with right-sided heart failure):
- Grade 1: 0-2 mm indentation and rebounds immediately
- Grade 2: 3-4 mm indentation and rebounds within 15 seconds
- Grade 3: 5-6 mm indentation and rebounds within 30-60 seconds
- Grade 4: 8mm or more indentation and rebounds 60 seconds or longer
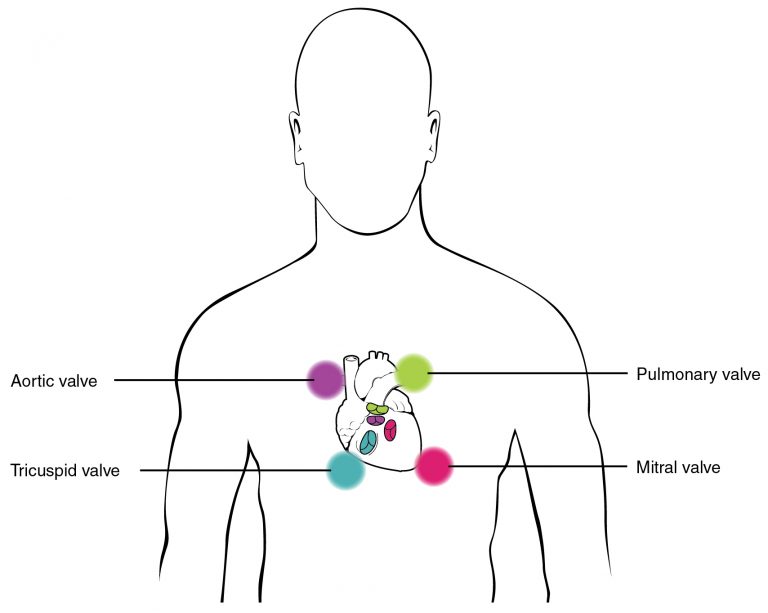
Auscultation of heart sounds
- S1:
- Normal heart sound
- First heart sound when atrioventricular (mitral and tricuspid) valves close
- Heard at the 5th intercostal space at the midclavicular line
- Signals the beginning of systole
- Often referred to as “lub”
- S2
- Normal heart sound
- Second heart sound when semilunar (aortic and pulmonary) valves close
- Heart at the second intercostal space along the right sternal border
- Signals the beginning of diastole
- Often referred to as “dub”
- S3
- Adventitious heart sound in adults and normal in children- Any extra sounds should be reported to the the supervising therapist.
- Heard between the 4th and 5th ribs on left side of chest
- Associated with rapid filling of ventricles during early diastole
- Often associated with fluid overload or a weakened left ventricle, which can be indicative of heart failure, myocardial infarction, dilated cardiomyopathy, valvular regurgitation, or constrictive pericarditis
- S4
- Adventitious heart sound in adults and children- Any extra sounds should be reported to the the supervising therapist
- Heard between the 4th and 5th ribs on the left or right side of the chest
- Associated with reduced ventricular compliance or increased resistance to ventricular filling
- Often associated with left ventricular hypertrophy or left-sided heart failure