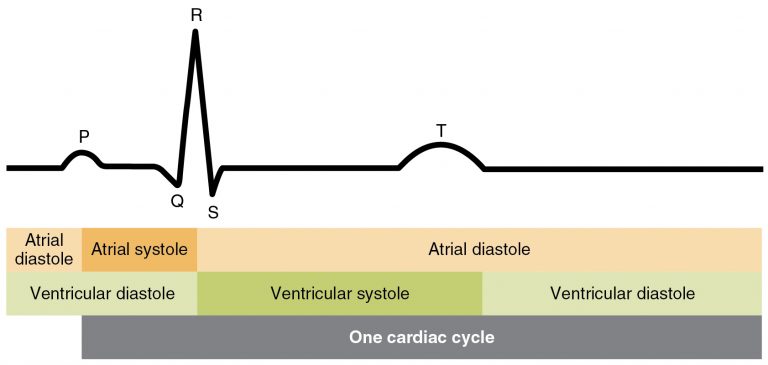




Electrocaradiograms
How to read electrocardiograms
Important considerations for reading electrocardiograms
- Is the rhythm regular and consistent?
- Is the rate fast, slow, or normal?
- Are P waves present and look the same?:
- Is the PR interval normal and consistent?
- Are the QRS complexes normal and immediately follow the P wave?
- Is the T wave present and normal in appearance?
- When viewing a multiple lead EKG strip view lead II or the line where the pattern can be defined clearly.
- Inverted waves are a polarity reversal often from improper lead placement, It is important to focus on the pattern listed above 1-6.
Calculation of heart rate with EKG
Calculation of heart rate using an EKG should only be done when the rhythm is consistent and predictable, allowing for easy calculations.
Calculations as follows for a 6-second strip method:
Count the number of QRS complexes in 6 seconds and multiply by 10
Example:
7 QRS peaks noted in 6 seconds x 10 = 70 bpm (heart rate). This is in the normal range of 60-100.
Common EKGs
Sinus bradycardia (slow heart rate, below 60 beats per minute at rest)
PT implications:
- Common to see this rhythm when working with those taking beta-blockers and in the elderly population
- If present, ok to proceed with initiation of activity and continuance of activity,
- Will need to use the perceived exertion scale (RPE)to assess tolerance to activity
- Monitor for symptoms of dizziness, lightheadedness, and pallor
Sinus tachycardia (fast heart rate), > 100 beats per minute at rest)
PT implications:
- Common to observe this rhythm during exercise
- Pay attention if the individual develops a headache, dizziness, or lightheadedness with tachycardia
- If these symptoms present, the therapist will stop the activity and reassess all vitals
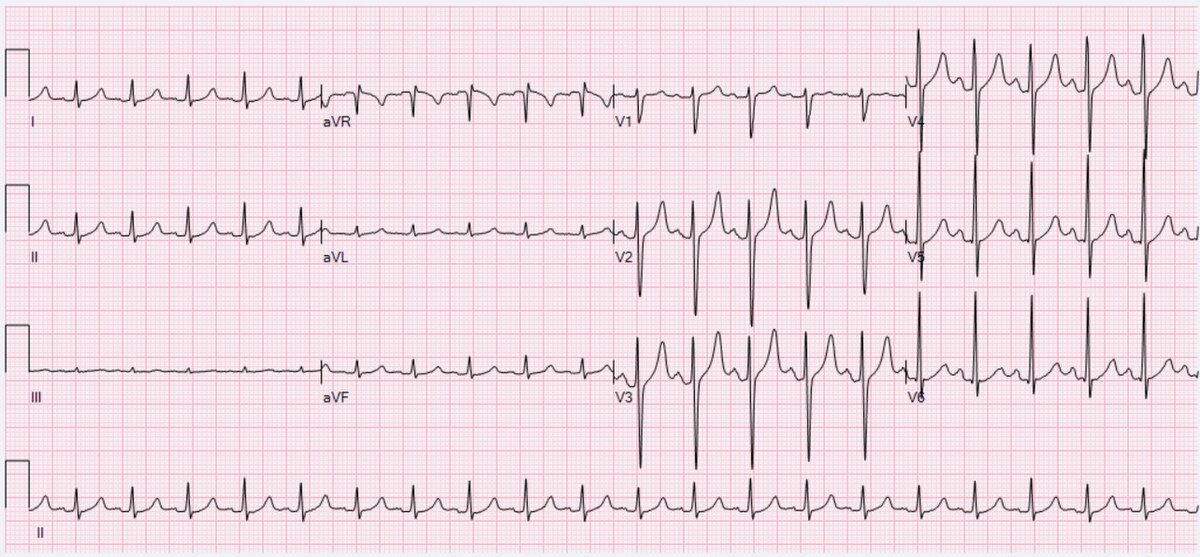
A-fibrillation (A-fib)
PT implications
If not previously recognized, stop activity and notify
If identified previously:
- Vital sign monitoring
- Continuous or frequent monitoring of heart rate, blood pressure, and oxygen saturation is essential.
- Pulse may be irregular, so use auscultation or ECG for accuracy rather than the radial pulse alone.
- Be aware that heart rate may be elevated or vary unpredictably.
- Exercise prescription
- Begin with low to moderate intensity activities; avoid high-intensity or sudden exertion early in rehab.
- Use Rate of Perceived Exertion (RPE) rather than heart rate alone due to variability.
- Monitor for signs of exercise intolerance: dizziness, fatigue, palpitations, chest pain, or dyspnea.
A-flutter
PT implications
If not previously recognized, stop activity and notify
If identified previously:
- Vital sign monitoring
- A-flutter often presents with a regular but rapid atrial rate (240–400 bpm); ventricular response may be regular or irregular depending on AV block.
- Carefully monitor heart rate and rhythm, as patients may suddenly shift into more dangerous rhythms (e.g., atrial fibrillation or rapid ventricular response).
- Use ECG or telemetry when possible, especially in acute care settings.
- Exercise intensity and progression
- Initiate with low to moderate intensity aerobic activity.
- Use RPE scales to guide intensity because HR may not accurately reflect exertion, especially if rate-controlled.
- Avoid abrupt changes in activity that could increase sympathetic tone and trigger rhythm instability.
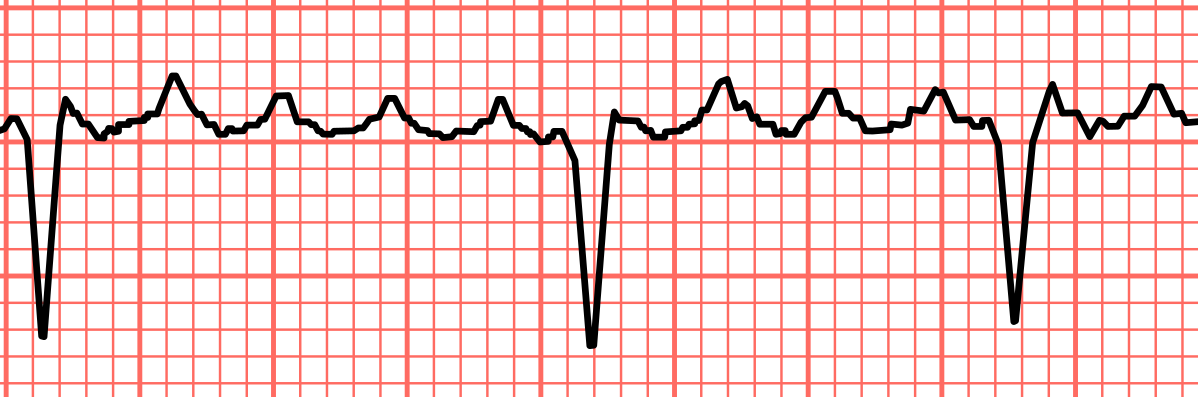
Premature ventricular contraction (PVC)
PT implications
- Singular PVC at rest and exercise: initiate or continue with activity, as this can be an anomaly
- Can be caused by stress, caffeine, or idiopathic
- Bigeminy (2) stop and rest x 5 min resume ex only if resolved,
- Three or more PVCs in a row at rest or with exercise: do not initiate activity and discontinue exercise, as this could lead to fatal heart rhythms
- Monitor for symptoms: heart fluttering, heart pounding, missed heartbeats
Ventricular tachycardia
PT implications
- Medical emergency and CPR initiated
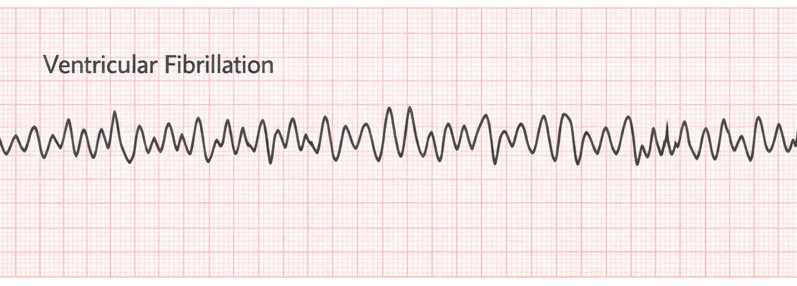
Ventricular fibrillation
PT implications
- Medical emergency and CPR initiated
Lab values
Lab values can be found at the American Physical Therapy Association (APTA) interpretation guide.
Vital signs
- Temperature: 97℉ - 99.6℉
- High value indicates fever
- Resting heart rate: 60-100 beats per minute
- Below 60 indicates bradycardia
- Above 100 indicates tachycardia
- Respiration: 12- 20 breaths per minute
- Below 12 indicates respiratory depression
- Above 20 indicates hyperventilation
- Blood pressure: 120/80
- See Chapter 2.1
- Oxygen saturation (O2 sats) 90%-100%
- Below 90% indicates possible need for supplemental oxygen
Hematological - Complete blood count
- Hemoglobin: responsible for transporting oxygen via red blood cells
- Male: 14-18
- Female: 12-16
- Below normal values indicate anemia, which increases the risk for blood transfusion
- An above normal value indicates polycythemia, which increases the risk for clogging of capillaries
- Hematocrit: ratio of red blood cells to total volume of blood
- Male: 42%-52%
- Female: 37%-47%
- Below normal values indicate anemia, which increases the risk for blood transfusion or need for fluids *An above normal value indicates polycythemia, which increases the risk for clogging of capillaries
- Platelets: clot-forming components of blood
- 150,000-400,000 mm3
- Below 150,000 mm3 indicates thrombocytopenia, which increases risk for hemorrhage, bleeding from gums, heavy menstrual bleeding, or blood in urine or stools
- Above 400,000 mm3 indicates thrombocytosis which increases risk for DVT development
- 150,000-400,000 mm3
- White blood count: important in immune response to infectious processes
- 5,000 - 10,000 mm3
- Below 5,000 mm3 indicates leukopenia which increases the risk for recurrent infections
- Above 10,000 mm3 indicates leukocytosis, which increases the risk for inflammation, immune system, or bone marrow disease
- 5,000 - 10,000 mm3
- Red blood count: cells that carry oxygen from the lungs to the tissue and are produced within the bone marrow
- Male: 4.7-6.1
- Female: 4.2-5.4
- Below normal values indicate anemia, which increases the risk for blood transfusion
- An above normal value indicates polycythemia, which increases the risk for myocardial infarction and stroke
- INR (international normalized ratio): the specific blood test used to measure the time it takes for blood to form a blood clot
- 0.8 – 1.2: normal range for a person not on anticoagulants
- Too Low (< 2.0): Blood may clot too easily → risk of thrombosis, stroke, or embolism.
- Too High (> 3.0–3.5): Blood is too thin → increased risk of bleeding, especially dangerous in falls or with trauma.
- 0.8 – 1.2: normal range for a person not on anticoagulants
Liver panel
- Albumin: A Protein that assists with moving small molecules such as bilirubin, progesterone, and calcium through the body
- 3-5.5
- Lab value that indicates nutritional status in the last 12-18 days
- Below 3 indicates malnutrition
- Will need to increase overall protein intake
- Above 55 indicates chronic kidney disease
- 3-5.5
- Pre-albumin: protein that assists with moving small molecules such as bilirubin, progesterone, and calcium through the body.
- 15-36
- Lab value that indicates nutritional status in the last 1.9 days
- This is the preferred lab value for nutritional status
- Below 15 indicates malnutrition
- Will need to increase overall protein intake
- Above 36 indicates chronic kidney disease
- Lab value that indicates nutritional status in the last 1.9 days
- 15-36
Renal function
- Blood urea nitrogen (BUN): Measures the metabolic function of the kidney and the excretory function of the kidney
- 10-20
- Below 10 indicates hepatic disease or issues with liver absorption
- Above 20 indicates a high protein diet, burns- overbody covering a large surface area due to increased metabolism occurring, septic shock
- 10-20
- Creatine kinase: Involved in the supply of energy for muscular contraction
- Male: 0.6-1.2
- Female: 0.5-1.1
- Below normal decreased muscle mass, debilitation
- Above normal renal disease, rhabdomyolysis, endocrine dysfunction
Cardiac lab values
- Troponin:
- Lab value indicates suspected acute coronary ischemic disease
- Troponin T: < 0.1
- Troponin: < 0.03
- Above normal: myocardial injury or myocardial infarction
- Lab value indicates suspected acute coronary ischemic disease
Arterial blood gases — see further explanation in later chapter 3.3
- pH: 7.35- 7.45
- Partial pressure of carbon dioxide (PaC02): 32-45
- Bicarbonate (HCO3): 22-26
Lipid panel
- Low density lipoprotein (LDL - bad cholesterol):
- Creates plaque and occlusions in blood vessels
- Normal <100
- Low level indicates decreased protein malabsorption, severe burns
- High levels indicate liver or kidney disease
- High density lipoprotein (HDL- good cholesterol):
- Helps to remove excess cholesterol deposits
- Normal: >60 mg/dL
- Below 35 mg/dL indicates increased risk for cardiovascular disease
- Triglycerides:
- Produced in the liver and transported to fatty tissue
- Desirable <150
- Above 150 is hypertriglyceridemia indicates an increased risk for hypothyroidism, myocardial infarction, or cardiovascular disease
- No specific value- hypotriglyceridemia indicates increased risk for malnutrition
- Total cholesterol:
- Main lipid associated with cardiovascular disease
- <200
- 200 or higher hypercholesterolemia indicates increased risk for cardiovascular disease
- No specific value- hypocholesterolemia indicates increased risk for malnutrition
- <200
- Main lipid associated with cardiovascular disease
Ankle brachial index (ABI)
- Procedure in which the systolic blood pressure is taken from the brachial artery (brachial) and the dorsalis pedis and posterior tibialis arteries (ankle) to assess if peripheral arterial disease is present
- Ratio of ankle blood pressure over brachial blood pressure
- Summary of Results:
- 1.4 and above:
- indicates calcification and vessel hardening
- 0.9-1.3:
- Normal, no disease present
- 0.51-0.89
- Arterial insufficiency- mild
- 0.5 and below:
- Arterial insufficiency- severe
- Lower extremity compression contraindicated
- Arterial insufficiency- severe
- 1.4 and above:
- Summary of Results:
- Ratio of ankle blood pressure over brachial blood pressure