
Inflammatory and degenerative disorders of bone
Osteoarthritis
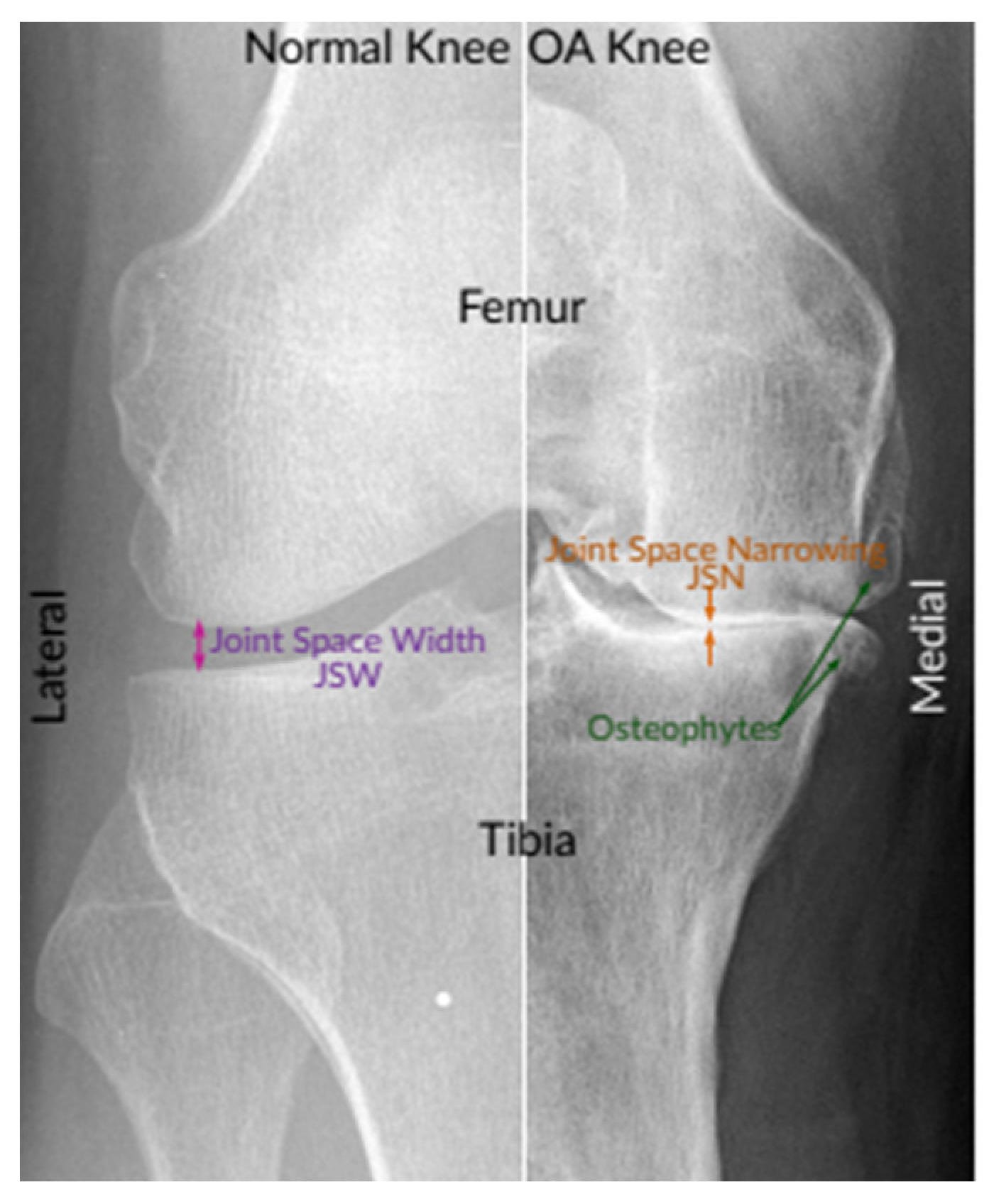
Osteoarthritis is a degenerative joint disease characterized by damage to articular cartilage, hypertrophy of bone (seen as osteophytes), subchondral bone sclerosis, and thickening of the joint capsule. Risk factors include genetics, female sex, past trauma, advancing age, and obesity. It’s more common after age 60. However, younger people can also develop osteoarthritis, especially with obesity, sedentary lifestyle, genetic cartilage defects, joint injury, or malalignment.
Inflammatory changes in the synovium and cartilage contribute to disease progression. Cytokines, chemokines, and other inflammatory mediators (such as nitric oxide) are produced, and proteinases are activated. Together, these changes lead to progressive damage of cartilage and synovium.
Osteoarthritis presents with:
- Joint pain that worsens with activity, especially after a period of rest (the “gelling phenomenon”)
- Morning stiffness lasting less than 30 minutes
- Joint locking and instability
It commonly affects the hands, knees, hips, and spine, typically with asymmetric involvement. The metacarpophalangeal joints are less likely to be involved. Swelling and deformity of the proximal and distal interphalangeal joints are called Bouchard and Heberden nodes, respectively. A popliteal cyst (Baker’s cyst) may occur.
X-ray findings include joint space narrowing, osteophytes, and subchondral cysts.
Gout
Gout is an inflammatory arthritis caused by deposition of monosodium urate crystals in and around joints. It’s more common in men, alcoholics, people with diets high in purine-rich foods (like meat) or high fructose corn syrup, and those with a family history of gout. Patients with chronic renal failure, metabolic syndrome, and Lesch-Nyhan syndrome are at higher risk. Medications such as diuretics, cyclosporine, low-dose aspirin, and niacin also increase risk.
Uric acid is derived from purine breakdown. Hyperuricemia due to decreased excretion and/or overproduction of uric acid predisposes to monosodium urate crystal formation. These crystals are needle-shaped and are ingested by neutrophils and macrophages, which leads to secretion of pro-inflammatory cytokines such as IL 1 and TNF alpha.
The disease presents as “flare ups” of acute gout with intense pain, swelling, and redness in and around joints. Attacks are often triggered by food, medications, trauma, and illnesses. Acute gout affecting the first metatarsophalangeal joint (great toe) is called podagra.
In chronic gout, tophi form in bone, cutaneous tissues, and articular spaces. Tophi are deposits of monosodium urate crystals in soft tissue. Long-term damage can cause joint deformity. Renal calculi may form.
Intercritical gout refers to the asymptomatic period between gout attacks.
Diagnosis is based on clinical features and synovial fluid aspirate showing:
- Negatively birefringent, needle-shaped crystals
- Crystals that are yellow under parallel and blue under perpendicular light
- Increased neutrophil count
X-ray findings include “punched out” joint erosions surrounded by sclerotic changes and overhanging edges, with tophi in bone and surrounding soft tissue. Classically, there is no osteopenia and joint space is preserved.
Pseudogout
Pseudogout is an inflammatory joint disease caused by deposition of CPPD (calcium pyrophosphate dihydrate) crystals. It’s seen in older age and affects both men and women.
The knee joint is most commonly involved. Clinical features are similar to gout, and chondrocalcinosis is present. CPPD crystals are rhomboid-shaped and weakly positively birefringent, appearing blue on parallel polarized light. Treatment is similar to gout.
Rheumatoid arthritis
Rheumatoid arthritis (RA) is a chronic, systemic, autoimmune inflammatory disorder that affects joints and, in some cases, the skin, heart, lungs, and eyes. Women are more commonly affected.
Autoantibodies include:
- Rheumatoid factor (an IgM antibody against IgG)
- Anti- CCP (cyclic citrullinated peptide) antibodies
Tissue destruction is mediated by T cells, neutrophils, and macrophages. Interleukins such as TNF alpha, IL 1, 6, and 8 are elevated. RA has a strong association with HLA DR4.
RA presents with joint pain and stiffness lasting more than 30 minutes. It usually affects small joints of the hands and feet (except the DIP joint), as well as the knees, cervical spine, and ankle joints. Joint damage can cause deformities such as Swan-neck and boutonniere deformities. Subcutaneous rheumatoid nodules are seen over extensor surfaces.
Systemic involvement can occur, including inflammation of the cervical spine, heart, kidney, etc. Patients are at risk for atlanto-axial subluxation.
Anti-CCP antibody is the most sensitive and specific test. Rheumatoid factor is elevated in about 75% of patients. X-rays show periarticular erosions, joint space narrowing, and osteopenia.
A Baker’s cyst may form in the popliteal fossa behind the knee. It’s a fluid-filled cyst and may rupture, resembling thrombophlebitis.
Treatment of rheumatoid arthritis includes NSAIDs, steroids, methotrexate, antimalarials, leflunomide, sulfasalazine, etc. Several biologics are used, including etanercept, infliximab, adalimumab, anakinra, rituximab, and tocilizumab.
Syndromes related to rheumatoid arthritis
- Felty’s syndrome - RA with splenomegaly and leukopenia
- Still’s disease - RA with acute onset, fever, rash and splenomegaly
Ankylosing spondylitis
Ankylosing spondylitis is an inflammatory arthritis affecting the hip joint, vertebrae, ribs, shoulders, knees, ankles, and feet. Risk factors include family history, age < 45 years, male sex, Crohn’s disease, ulcerative colitis, or psoriasis. Uveitis may be seen. There is a strong association with HLA B 27.
It presents with lower back and/or hip pain and stiffness. Pain typically worsens during rest or inactivity and improves with movement and exercise. X-ray shows bamboo spine.
Chondromalacia
Chondromalacia, commonly called chondromalacia patellae or runner’s knee, is a common cause of anterior knee pain among young people, especially young women who participate in sports.
The initial pathological change in CMP is that cartilage becomes dull or slightly yellowish-white, then soft, swollen, and edematous in the early stage, followed by fragmentation or erosion of cartilage in advanced stages.
It presents with anterior knee pain that worsens with squatting, climbing stairs (up or down), running, or prolonged sitting. It can lead to osteoarthritis of the knee. On exam, retropatellar crepitus is present.
X-ray is not sensitive; MRI or arthroscopy is used for diagnosis. Management is conservative (activity restriction, physiotherapy, pain management). Surgical therapy includes partial or complete patellectomy.
Disc prolapse
Disc prolapse is caused by degenerative disease of the intervertebral disc. The intervertebral disc is composed of three layers:
- fibrous annulus with its outer and inner part
- central pulposus nucleus
- terminal plates
Disc herniation (prolapse) is bulging of the disc due to partial or complete rupture of the outer fibrous annulus. The bulge may be anterior, posterolateral, or posterior. The most common location is L4/5, followed by L5/S1.
Key risk factors include heavy physical labor, smoking, obesity, inappropriate flexed posture, and lack of physical activity. Men between ages 20 and 50 are most likely to have a herniated disk.
Symptoms include:
- Low back pain
- Sharp, shooting, or burning pain extending from the buttock down the back of one leg (sciatica)
- Numbness or tingling and/or weakness in the leg and/or foot
Pain decreases with standing and increases with bending and sitting. The straight leg raising (SLR) test is positive in lumbar disc prolapse. Pain reproduced between 30-70 degrees of hip flexion suggests disc herniation at L5-S1 or L4-L5.
CT and MRI can reveal the level and degree of herniation. X-ray shows narrowed intervertebral disc spaces. Myelography localizes the site of disc herniation and the presence of root entrapment.
Management of uncomplicated disc herniations includes rest, physical therapy, and anti-inflammatory and analgesic medications. Persistent symptoms may benefit from corticosteroid injections. Operative therapy includes laminectomy or discectomy.
Evaluation of Pain during the SLR test
| Degree of flexion at hip | Inference |
| <30 degrees | Spondylolisthesis, gluteal abscess, inflammation of the dura mater, malingering |
| 30-70 degrees | Disc herniation at L5-S1 or L4-L5 |
| >70 degrees | Tight hamstrings or gluteus maximus, pathology of the hip or sacroiliac joints |
Cauda Equina Syndrome
The cauda equina is a bundle of spinal nerves consisting of lumbar and sacral spinal nerves and the coccygeal nerve. It resembles a horse’s tail, which is where the name comes from.
Collectively, the cauda equina nerves innervate pelvic organs and the lower limbs, including the internal and external anal sphincters, perineum, bladder parasympathetics to the detrusor muscle (via the pelvic splanchnic nerves), and motor supply to the lower limb.
Any lesion that compresses the cauda equina - such as disc herniation, spinal stenosis, spinal trauma, local ependymomas and schwannomas, or metastatic tumors - can cause cauda equina syndrome.
It presents with low back pain, sciatica, saddle anesthesia in the perineal area, lower limb paresis with hyporeflexia, and bowel/bladder incontinence. It is a surgical emergency and should be treated with immediate surgical decompression.
Spondylolisthesis and spondylosis (degenerative)
Spondylolisthesis and spondylosis are degenerative disorders of the vertebrae. Spondylosis is a weakening or defect in the pars interarticularis. Spondylolisthesis is anterior displacement of a vertebra, which occurs due to spondylosis.
It occurs most commonly due to repetitive stress and microtrauma and is more common in women over age 40. It most commonly affects the L4-5 or L5-S1 vertebral levels.
Symptoms include low back pain, buttock and posterior leg pain aggravated by walking and relieved by sitting and rest, and signs of radiculopathy such as weakness in dorsiflexion. Complications include spinal stenosis and cauda equina syndrome.
AP and lateral X-rays show anterior subluxation or displacement of the vertebral body over the adjacent one. First-line therapy includes NSAIDs and physical therapy, with epidural steroid injections in resistant cases. Surgical management is decompression surgery.