Hormones and their role in exercise
Testosterone
Testosterone is the primary androgenic hormone involved in skeletal muscle growth and remodeling. It supports muscle protein synthesis, neuromuscular function, and recovery after resistance training. The testosterone response to exercise is typically acute and transient. Long-term adaptations depend not only on circulating hormone levels, but also on androgen receptor sensitivity.
Key functions of testosterone in exercise:
- Enhances protein synthesis and muscle fiber repair.
- Increases neurotransmitter release, promoting greater motor unit activation.
- Regulates anabolic processes that support hypertrophy and performance.
- Binds to androgen receptors on muscle cells to activate muscle growth.
Factors affecting testosterone response:
- Exercise selection: Large muscle group exercises (e.g., squats, deadlifts) elicit greater testosterone responses.
- Training intensity: Moderate to high volume resistance training (85-95% of 1RM) stimulates higher testosterone levels.
- Rest intervals: Shorter rest periods (30 seconds to 1 minute) can enhance hormonal response.
- Training experience: Individuals with more training years exhibit more robust hormonal adaptations.
Free vs. bound testosterone
Testosterone circulates in both bound and free forms. Bound testosterone is attached to proteins such as sex hormone-binding globulin (SHBG) or albumin. Free testosterone is not bound to these proteins, so it’s more readily available to interact with muscle cells. Resistance training can temporarily increase free testosterone, which may enhance its anabolic effects.
Testosterone responses in women
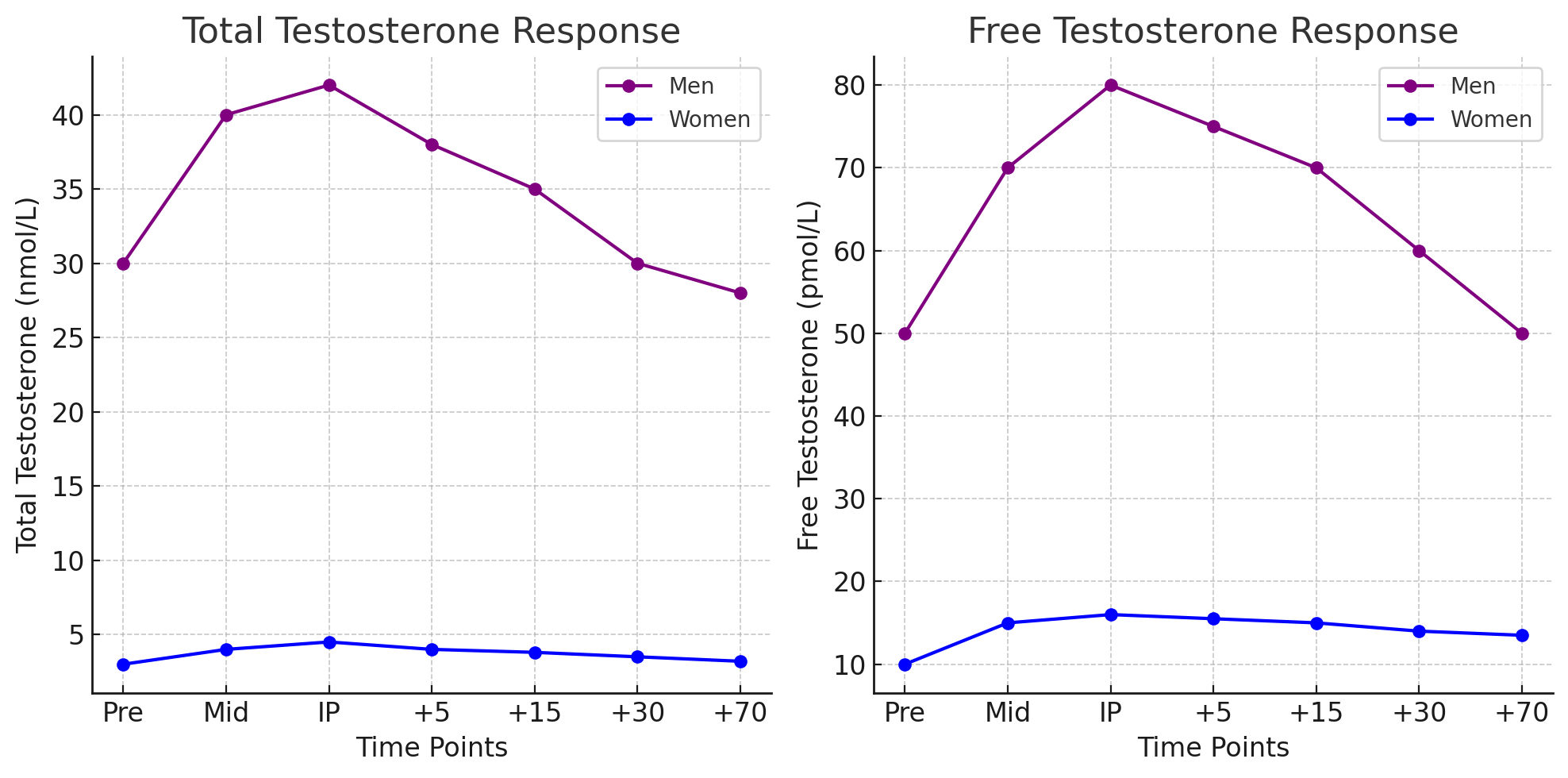
Women have much lower circulating testosterone (about 15- to 20-fold less than men), but resistance training can still produce small, meaningful changes. Most studies report no acute rise in total testosterone in women after exercise. However, some findings suggest that free testosterone may increase with high-volume, multi-set resistance exercise.
Total Testosterone (nmol/L) and Free Testosterone (pmol/L) responses to six sets of squats at 80% of 1RM with 2 minutes of rest between sets. The Midpoint (Mid) sample taken after three sets.
Growth hormone
Growth hormone (GH) contributes to muscle growth, metabolism, and broader physiological adaptations to resistance training. It’s secreted primarily by the anterior pituitary gland and exists in several molecular forms. The 22 kDa variant is the most commonly studied.
Physiological functions of growth hormone:
GH affects many target tissues. Key effects include:
- Decreases glucose utilization, promoting greater reliance on fatty acids for energy.
- Increases amino acid transport across cell membranes, supporting protein synthesis.
- Promotes lipolysis, breaking down fat stores for energy.
- Increases collagen synthesis, supporting joint and connective tissue health.
- Enhances immune cell function, supporting recovery and adaptation.
- Stimulates cartilage and bone growth, which supports long-term training adaptations.
- Increases renal plasma flow, assisting in fluid balance and recovery.
Regulation of GH secretion
GH secretion is controlled by neuroendocrine feedback mechanisms, including:
- Hypothalamus: Releases growth hormone-releasing hormone (GHRH), which stimulates GH secretion.
- Somatostatin: Inhibits GH release to prevent excessive levels.
- Peripheral feedback: Insulin-like growth factors (IGFs) released by the liver provide negative feedback to regulate GH output.
Exercise variables influencing GH release:
- Exercise intensity and volume: Higher intensity (70-85% of 1RM) and multiple sets elicit greater GH responses.
- Rest intervals: Shorter rest periods (e.g., ≤1 minute) result in higher GH concentrations compared to longer rest intervals.
- Metabolic stress: GH secretion correlates with lactate production and the degree of metabolic challenge induced by exercise.
- Training status: Trained individuals may experience more efficient GH responses due to improved receptor sensitivity.
- Age: GH secretion declines with age, which can affect hypertrophy potential.
Functions of growth hormone in exercise:
- Stimulates protein synthesis and muscle repair.
- Mobilizes free fatty acids for energy during exercise.
- Enhances collagen synthesis, supporting connective tissue integrity.
- Works synergistically with other anabolic hormones like insulin-like growth factor-1 (IGF-1).
Gender differences in GH response:
Women typically have higher baseline GH levels than men, influenced in part by hormonal fluctuations across the menstrual cycle. Research suggests:
- During the follicular phase, women experience higher GH concentrations than in the luteal phase.
- Exercise-induced GH responses are more pronounced with higher exercise intensity and shorter rest periods.
Hormonal adaptations over time
With long-term resistance training, the endocrine system shows both acute and chronic adaptations that improve the body’s ability to manage exercise stress. Common adaptations include:
- Increased baseline hormone levels: Regular training can increase resting concentrations of anabolic hormones such as testosterone and GH.
- Enhanced receptor sensitivity: Muscle cells become more responsive to hormone signaling.
- Reduced catabolic effects: Training can suppress excessive cortisol release, which helps limit muscle breakdown.
- Greater hormone efficiency: The endocrine system becomes more effective at managing hormonal fluctuations.
Insulin-like growth factors (IGFs)
Insulin-like growth factors (IGFs) help mediate many anabolic effects associated with GH by promoting muscle protein synthesis and cellular growth. The liver produces most circulating IGF-1 in response to GH, but skeletal muscle can also produce IGF-1 locally through GH-independent pathways.
Roles of IGFs in exercise adaptations:
- Stimulates muscle hypertrophy by increasing protein synthesis.
- Facilitates recovery by promoting satellite cell activation.
- Enhances glucose uptake, improving energy availability for training.
- Regulates autocrine and paracrine signaling in muscle tissue, driving localized muscle growth.
Binding proteins and IGF availability
In circulation, IGFs bind to specific binding proteins (e.g., IGFBP-3). These proteins regulate IGF bioavailability and help transport IGFs to target tissues. Factors that influence IGF function include:
- Training intensity and volume: Higher workloads can upregulate IGF production.
- Nutritional status: Adequate protein and carbohydrate intake supports IGF responses.
- Hormonal interactions: GH, insulin, and thyroid hormones influence IGF activity.
Exercise responses of IGF-1:
- Acute response: Immediate post-exercise increases are often observed with resistance training.
- Chronic adaptation: Long-term training can lead to sustained elevations in IGF-1, contributing to muscle hypertrophy.
Training adaptations of GH and IGFs
With consistent resistance training, GH and IGF-1 secretion can adapt in ways that support muscle growth and metabolic efficiency.
Key adaptations observed:
- Increased baseline levels: GH and IGF-1 levels rise at rest with chronic training.
- Improved muscle sensitivity: Target tissues become more responsive to hormonal signaling.
- Reduction in catabolic hormones: Lower cortisol levels help preserve muscle mass.
Training recommendations for optimizing GH and IGF-1 response:
- Utilize high-intensity resistance training with short rest intervals.
- Incorporate progressive overload to maintain hormonal stimulation.
- Ensure adequate recovery to prevent hormonal desensitization.
Mechanisms of hormonal transport and clearance
Hormones produce their effects through coordinated transport and clearance processes:
- Synthesis and storage: Hormones are synthesized and stored in glands until exercise-related signals trigger release.
- Transport via binding proteins: Many hormones, such as testosterone, circulate bound to proteins like SHBG.
- Receptor affinity: Hormones must bind to specific receptors to act; receptor availability and affinity can change with training.
- Clearance and degradation: Hormones are metabolized and cleared by the liver and kidneys, which affects how long they remain active.
Cortisol: The primary catabolic hormone
Cortisol is a glucocorticoid hormone released by the adrenal cortex in response to stress, including resistance training. Although cortisol is often described as purely catabolic, it has an important acute role in mobilizing energy and managing stress. Problems arise when cortisol remains chronically elevated, because this can impair recovery and adaptation.
Functions of cortisol:
- Promotes gluconeogenesis, converting amino acids into glucose for energy.
- Inhibits protein synthesis, which can contribute to muscle breakdown if chronically elevated.
- Suppresses immune function, helping regulate inflammation.
- Regulates fat metabolism, promoting lipolysis during prolonged exercise.
Exercise responses of cortisol:
- Acute increases: Resistance training - especially high volume with short rest intervals - can cause transient spikes in cortisol.
- Chronic adaptations: Over time, well-structured training can reduce baseline cortisol and improve anabolic-to-catabolic balance.
- Sex differences: Women typically show greater cortisol responses than men, although receptor sensitivity and metabolic adaptations may differ.
Cortisol and resistance training adaptations:
- The testosterone-to-cortisol ratio (T:C ratio) is often used as an indicator of an athlete’s anabolic or catabolic state.
- Training-induced cortisol responses should be monitored to reduce the risk of overtraining and excessive muscle breakdown.
- Proper nutrition (adequate protein and carbohydrate intake) can help reduce cortisol’s negative effects on muscle tissue.
Catecholamines and their role in exercise
The adrenal medulla secretes the catecholamines epinephrine, norepinephrine, and dopamine. These hormones drive many of the body’s immediate responses to exercise. They prepare you for high-intensity effort by rapidly mobilizing energy and supporting performance. Catecholamines can also stimulate other anabolic hormones, including testosterone and growth hormone, which further support training adaptations.
Key functions of catecholamines:
- Increase force production by enhancing neural drive.
- Elevate energy availability by mobilizing glycogen and fat stores.
- Increase cardiac output, improving oxygen and nutrient delivery to muscles.
- Enhance metabolic enzyme activity, supporting ATP production.
- Stimulate other anabolic hormones, such as testosterone and growth hormone.
Training adaptations of catecholamines:
- Increased secretory capacity: Repeated high-intensity training improves the adrenal gland’s ability to produce catecholamines.
- Faster recovery: Well-conditioned athletes clear catecholamines more efficiently, reducing stress and improving readiness for the next session.
- Reduced stress response: Chronic training can produce more efficient responses to physical stressors, limiting excessive hormonal spikes.
Optimal training strategies for catecholamine release:
- High-intensity training with short rest intervals enhances catecholamine release.
- Multi-joint compound exercises stimulate greater hormonal responses.
- Gradual exposure to higher training loads improves the efficiency of catecholamine function.
Practical considerations
To maximize endocrine adaptations from resistance training, consider the following strategies:
Increasing testosterone levels:
- Utilize compound exercises (squats, deadlifts, power cleans).
- Train at 85-95% of 1RM with multiple sets and short rest periods (30-60 seconds).
- Maintain consistent high-volume training over at least two years.
Enhancing growth hormone secretion:
- Incorporate higher lactate-producing exercises, such as high-rep sets with short rest.
- Ensure a protein-carbohydrate intake pre- and post-workout to support GH release.
- Use progressive overload, increasing intensity systematically over time.
Optimizing adrenal hormone function:
- Vary training protocols to reduce the risk of adrenal exhaustion and non-functional overtraining.
- Implement periodization with alternating periods of high and low intensity to allow hormonal recovery.
- Monitor fatigue levels and adjust workload to maintain endocrine balance.
Hormonal regulation of muscle hypertrophy:
Hormonal adaptations to resistance training contribute to muscle hypertrophy through several related processes:
- Muscle fiber recruitment: Hormones support greater motor unit activation, which improves force production.
- Protein turnover: Anabolic hormones like testosterone and GH increase protein synthesis while reducing protein breakdown.
- Satellite cell activation: Hormonal signaling helps regulate muscle regeneration by activating satellite cells.
- Energy mobilization: Hormones such as cortisol and epinephrine provide energy during exercise, but they must be managed to avoid excessive catabolism.
Considerations for strength coaches
To optimize endocrine responses to resistance training, strength coaches should:
- Tailor exercise selection: Prioritize multi-joint movements that engage large muscle groups.
- Manipulate rest intervals: Use shorter rest periods to maximize hormonal responses.
- Optimize nutritional strategies: Adequate protein and carbohydrate intake to support anabolic hormone production.
- Monitor training load: Avoid overtraining, which can negatively impact hormonal balance.
- Manipulating training variables: Adjusting intensity, volume, and rest to optimize hormonal responses.
- Recovery optimization: Ensuring sufficient sleep and stress management to regulate cortisol levels.
- Monitoring biomarkers: Tracking hormone levels as indicators of overtraining or recovery status.
Other hormonal considerations
Several other hormones interact with the endocrine system and contribute to exercise adaptations:
- Insulin: Facilitates glucose uptake and glycogen storage post-exercise, supporting recovery and muscle growth.
- Thyroid hormones (T3, T4): Regulate metabolic rate and energy expenditure.
- Beta-Endorphins: Help manage pain and stress during prolonged exercise.
Adrenal hormones and their role in exercise:
The adrenal glands play a key role in the body’s response to exercise stress. They have two main parts:
- Adrenal medulla: Secretes catecholamines such as epinephrine, norepinephrine, and dopamine in response to immediate stressors (fight-or-flight response).
- Adrenal cortex: Produces corticosteroids like cortisol, which regulate metabolism and inflammation.